J Adv Periodontol Implant Dent. 18(1):11-19.
doi: 10.34172/japid.026.3806
Original Article
Assessment of gingival characteristics by professional versus smartphone imaging
Mohan Kumar Pasupuleti Conceptualization, Project administration, Resources, Supervision, Writing – original draft, Writing – review & editing, 1, * 
Gurramkonda Sirisha Investigation, Methodology, Writing – original draft, 2
Gabu Pujitha Investigation, Methodology, Writing – original draft, 2
Gautami Subhadra Penmetsa Resources, Validation, Writing – review & editing, 1
Supraja Salwaji Data curation, Formal analysis, 3
Nissi Gurindapalli Data curation, Supervision, 4
Author information:
1Department of Periodontics, Vishnu Dental College, Vishnupur, Bhimavaram, West Godavari, Andhra Pradesh, India
2Vishnu Dental College, Vishnupur, Bhimavaram, West Godavari, Andhra Pradesh, India
3Department of Oral and Maxillofacial Pathology, Vishnu Dental College, Vishnupur, Bhimavaram, West Godavari, Andhra Pradesh, India
4Department of Orthodontics, Vishnu Dental College, Vishnupur, Bhimavaram, West Godavari, Andhra Pradesh, India
Abstract
Background.
Accurate evaluation of gingival health requires understanding inflammation as a sign of disease activity or healing. Only a few studies have examined the gingiva in depth using non-invasive imaging techniques. Therefore, this study assessed the accuracy of evaluating gingival parameters using professional (Canon EOS 1300D, Canon Inc., Japan) and smartphone (iPhone 15 Pro, Apple Inc., USA) cameras, with pre- and post-treatment photographs.
Methods.
Thirty-four patients with gingivitis were selected, and photographs were captured using professional and smartphone cameras. Gingival parameters were examined using pictures of the maxillary anterior region taken at distances of 24, 28, and 32 cm from the examination site. All the images were evaluated using the free ImageJ software (US National Institutes of Health, Bethesda, Maryland, USA) with an accuracy of 0.01 mm. The paired t-test was used to compare gingival color values and clinical measurements. A P value of<0.05 was considered statistically significant.
Results.
There were no significant differences in gingival parameters between images taken using either professional or smartphone photography. The results showed no significant differences in gingival color assessment at 24-, 28-, and 32-cm distances between the two images.
Conclusion.
Digital images obtained with DSLR and smartphone cameras showed comparable accuracy for gingival parameter measurements at the tested distances.
Keywords: Colorimetry, Computer-assisted photography, Image processing, Smartphone
Copyright and License Information
© 2026 The Author(s).
This is an open access article distributed under the terms of the Creative Commons Attribution License (
http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Funding Statement
This research received no specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Introduction
The evaluation of gingival health has typically been based on clinical probing, visual inspection, and colorimetric assessment. Currently, clinical probing with a calibrated periodontal probe remains the gold standard for measuring sulcus depth, clinical attachment, and bleeding on probing; however, it is invasive, technique-sensitive, and often uncomfortable for the patient. Visual inspection is non-invasive, clinically user-friendly, and therefore easy for the clinician to identify inflammation, edema, and hypertrophy. Despite being non-invasive, visual inspection remains subjective and less reliable in the early stages of gingivitis, and the diagnosis may very well rely on the examiner’s experience.1,2
To consider quantitative structure, colorimetric assessments similar to all indices, including the modified gingival index (MGI), assess changes in gingival color and texture, which indicate inflammatory status. Although colorimetric indices do provide standardized criteria (e.g., scores based on redness or bleeding), they still rely on clinicians’ interpretation of color and are subject to variability. Other, more objective techniques include transgingival probing (which measures gingival thickness through probe transparency), which is quantitative but invasive, and ultrasound imaging or CBCT; all are objective and provide non-invasive exact numbers but come at a higher cost and are more complex, or, in the example of CBCT, expose patients to radiation.1,2
Dental practitioners must have anatomical knowledge of the periodontium, including its size, composition, and orientation, to understand the pathophysiology and aesthetics of the periodontal and surrounding tissues. The attached gingiva (AG) and keratinized gingiva (KG) exhibit distinct histological and morphological features. Collagen fibers securely link AG to the root cementum and alveolar bone, while KG is a combination of AG and the outer surface of the periodontal pocket or the bottom of the gingival sulcus.3,4
Prior research often employed a caliper and a periodontal probe to measure the gingival dimensions. The state of the periodontium, the expertise level, interference from nearby anatomic structures during measurement, and the set graduations on measuring instruments are among the potential drawbacks of various measurement techniques. The extensive use of digital technology in dentistry today offers a novel opportunity to address the aforementioned constraints.5,6
The assessment of gum health has historically been viewed as a fundamental aspect of comprehensive dental care because of its direct connection to overall oral health and its role in preventing various dental diseases. The gums, known as the gingiva, serve as a protective shield for the teeth and the supporting bone structures, and their well-being is essential for maintaining the functional and esthetic integrity of the mouth.7-9
The advancement of non-invasive methods for evaluating gingival health is a hopeful area of dental research. Historically, assessing gingival health has relied on clinical methods such as visual inspection, periodontal probing, and radiographic imaging, which, while useful, may be invasive, uncomfortable for patients, and prone to error. Furthermore, these traditional procedures need direct contact with the gums, which can cause discomfort (e.g., bleeding or pain while probing), especially in individuals with sensitive or previously inflamed tissues.9,10
Non-invasive diagnostic approaches, on the other hand, have the potential to alleviate some of these limitations by providing a more pleasant, effective, and patient-centered approach to monitoring gingival health. Despite the apparent advantages, research in this field is limited, and the non-invasive approach has not yet demonstrated clinical feasibility. Several factors have contributed to that, including the complexity of gingival disease, limitations in current technology, and the need for a comprehensive evaluation of a new approach.11-13
Thus, digital technologies can improve anatomical information. The goal of the current study was to compare gingival dimensions obtained from smartphone and DSLR (digital single-lens reflex) camera digital photos with those obtained by conventional clinical measurements using probes and by eye inspection for color evaluation.
Methods
The protocol of the present cross-sectional observational study was approved by the institutional Ethics Committee of Vishnu Dental College under reference number IECVDC/24/F/PI/IVV/49. The study was conducted between April and June 2024.
The inclusion criteria for the study were (1) volunteers affiliated with Vishnu Dental College, (2) age of ≥ 20 years, (3) satisfactory oral hygiene, defined by a full-mouth plaque index of < 20% and a full-mouth bleeding index of < 20%, and (4) no missing teeth. The exclusion criteria included (1) a history of orthodontic treatment, (2) mal-aligned dentition, and (3) current periodontal disease or a history of periodontitis.
In the study, 34 patients diagnosed with gingivitis were selected as participants to investigate their gingival health. Gingivitis is a common, mild form of periodontal disease characterized by inflammation of the gums, usually caused by plaque buildup at the gingival line. If left untreated, it can lead to more serious periodontal disease. The choice of these individuals allows us to concentrate research on gingival problems that are still in the early stages, without causing further damage to tissues found during periodontitis.
Patient selection
The patients were carefully selected based on specified inclusion criteria, which most likely included gingivitis but no other severe forms of gingival disease (such as periodontitis). This guaranteed that the research was limited to early-stage gingivitis, which can be effectively treated or reversed with good dental hygiene. The patients were also required to have acceptable oral hygiene (e.g., low plaque and bleeding indices) to prevent confounding variables in assessing gingival health.
Gingival clinical parameters and gingival color accuracy were examined using pictures of the maxillary anterior region taken at distances of 24, 28, and 32 cm from the examination site. Patients’ photographs were taken at 24, 28, and 32 cm with a DSLR camera and a smartphone.
Photographic image capture and lens selection
To assess the condition of the patients’ gums, photographs were captured using both professional cameras and smartphone cameras. Photographs were taken using a DSLR camera and an iPhone 15 Pro. Dental photographs were taken in this study with a professional camera using a Canon 18–55 mm kit lens, rather than a macro lens such as the Canon 100 mm macro lens typically recommended for standardized dental photography. This justification is based on availability. Lens selection can affect image magnification, distortion, depth of field, and the reproduction of fine gingival details. We acknowledge that the photographic parameters may have been affected by using a kit lens and will take this potential impact into account when reviewing the results.
Lighting conditions
Intraoral photographs were taken using the camera’s built-in pop-up flash as the primary light source. The flash was positioned directly over the lens to allow for frontal lighting. Due to the lack of directional or diffused lighting, this method can sometimes produce uneven lighting, glare, or shadows, especially from the lips over the maxillary anterior area. There were no external flash units, ring flashes, or diffusers used during this procedure. These lighting conditions were taken into account when interpreting color accuracy and morphometric measurements from the images.
Professional camera images
Professional cameras produce high-resolution, complex images and can capture small details of gum inflammation, such as redness, swelling, bleeding, and plaque. They also provide improved control of the lighting that guarantees a homogeneous and transparent image without fluctuating with natural light. Moreover, these cameras provide standardization by ensuring images are captured under ideal conditions, including uniform angles, magnification, and lighting, which is vital for precise, accurate assessments of gingival health (Figure 1).
Smartphone camera images
Although smartphone cameras usually have lower resolution than professional cameras, their availability and user-friendliness make them useful tools for taking photos in less regulated environments, such as dental offices. Their combination with mobile apps and editing software enables clinicians to conduct real-time evaluations, resulting in speedier documentation and image sharing. Furthermore, smartphone cameras allow for comparison studies to determine whether they can provide adequate image quality for clinical examinations, making them a viable and cost-effective alternative to specialized equipment in medical settings (Figure 2).
In this study, gingival clinical parameters and gingival color accuracy were examined by capturing photographic images of the maxillary anterior region (the upper front teeth and surrounding gingival tissues) before scaling and root planing, which are commonly performed to remove plaque and tartar from the teeth and below the gumline to treat gingivitis and early-stage periodontitis.
Image capture procedure
Images of the maxillary anterior area were captured at three designated distances from the examination location: 24, 28, and 32 cm. These different distances were selected to examine how the distance between the camera and the subject can affect the quality and precision of captured images. The study examined photos taken from various distances to identify the optimal distance for capturing gingival traits with the most detail and clarity. The decision to record photos at varying distances allows investigation of how distance affects image quality and depth of field, potentially influencing the precision of gingival color identification and the evaluation of clinical parameters (such as gingival redness, swelling, and tissue form).
Images were taken using both a smartphone and a DSLR camera. The DSLR camera, known for its high resolution and precise control over characteristics such as focus, lighting, and exposure, produces crisp, precise photos. In contrast, the smartphone camera is more convenient and accessible, and its performance was compared with that of the DSLR camera to determine whether it could produce results sufficiently accurate for clinical assessments.
Traditionally, the assessment of gingival color employed subjective terms, such as “pink” or “coral pink”, for example, which were unstandardized and nonreproducible. These qualitative terms were also subject to the investigator’s interpretation, clinical judgement, and even lighting conditions, which limited their clinical and research value. It was necessary to move to objective colorimetry because of the ability to view colors in different ways, and the CIELab color space (Commission Internationale de l’Éclairage Lab*, or short “CIE”) was a scientifically valid method of assessing gingival color through measurement of color in three axes: L: lightness as our first axis, a: red-green as our second axis, and b: yellow-blue as our third axis. CIELab provided an objective, precise, repeatable, and standardized means of measurement.
Post-procedure image examination
After photo capture, the images were analyzed using ImageJ, software developed by the U.S. National Institutes of Health. ImageJ enables accurate measurement of characteristics such as gingival color, width, and shape alterations. The software delivers measurements with a precision of 0.01 mm, enabling thorough examination of subtle variations in gingival health, including enhancements in gingival color and decreases in inflammation. Using ImageJ, clinicians can objectively measure important clinical factors, such as gingival margins, bleeding on probing, and plaque buildup, which aid in assessing the success of scaling and root planing and in monitoring the extent of gingival inflammation.
In this research, SPSS was employed to evaluate and contrast clinical data and gingival characteristics captured using professional and smartphone cameras. The objective was to determine whether statistically significant differences existed between the two imaging techniques for evaluating gingival health, particularly gingival color, margins, swelling, and various clinical characteristics.
Sample size calculation and statistical analysis
To compute the required sample size for a paired t-test (dependent means), an a priori power analysis was conducted with the following inputs: a two-tailed test, an effect size of dz = 0.5, an alpha error probability (α) of 0.05, and a desired power of 0.80 (1 - β). With these values, the crucial t-value was found to be 2.0345153, and the non-centrality parameter (δ) was found to be 2.9154759. After determining that there were 33 degrees of freedom (df), a total sample size of 34 individuals was required. This sample size yielded a real power of 0.8077775, which is comparable with the desired power of 0.80 and provides adequate statistical sensitivity to detect the impact. The study sought to statistically assess if there were significant variations in gingival color accuracy and clinical assessments at camera-to-patient distances of 24, 28, and 32 cm.
Results
The study used a combination of high-quality photographic imaging and precise image analysis software to assess gingival health and color accuracy before scaling and root planing. By using both DSLR and smartphone cameras and analyzing the images with ImageJ software, the research aimed to determine whether smartphone cameras could be used as a viable alternative to professional equipment in clinical settings for monitoring and evaluating gingival conditions, offering a cost-effective and accessible solution for dental professionals.
The gingival parameters measured were the width of KG, height of interdental papilla, gingival margin position, and width of attached gingiva at 24-, 28-, and 32-cm distances by using a DSLR camera and a smartphone.
Inter-group comparison: camera vs. smartphone at 24, 28, and 32 cm
The means and standard deviations (SD) of the width of KG measured digitally by both a DSLR camera and a smartphone were 5.7265 ± .60016 and 5.6118 ± .62122 at 24 cm, 5.5941 ± 0.64099 and 5.4941 ± 0.64099 at 28 cm, and 5.4265 ± .60016 and 5.3941 ± 0.64099 at 32 cm. The t-values and P-values of the width of KG measured digitally by both a DSLR camera and a smartphone were 0.774 and 0.442 at 24 cm, 0.643 and.522 at 28 cm, and 0.215 and 0.831 at 32 cm (Table 1).
The means and standard deviations (SD) of the height of interdental papilla measured digitally by both a DSLR camera and a smartphone were 2.4824 ± 0.43656 and 2.4088 ± 0.42737 at 24 cm, 2.3824 ± 0.43656 and 2.3088 ± 0.42737 at 28 cm, and 2.2824 ± 0.43656 and 2.2088 ± 0.42737 at 32 cm. The t-values and P values of the height of interdental papilla measured digitally by both a DSLR camera and a smartphone were 0.723 and 0.485 at 24 cm, 0.723 and 0.485 at 28 cm, and 0.723 and 0.485 at 32 cm (Table 1).
The means and standard deviations (SD) of gingival margin position measured digitally by both a DSLR camera and a smartphone were 0.4706 ± 0.78760 and 0.4706 ± 0.78760 at 24 cm, 0.4706 ± 0.78760 and 0.4706 ± 0.78760 at 28 cm, and 0.4706 ± 0.78760 and 0.4706 ± 0.78760 at 32 cm. The t-values and P values of the gingival margin position measured digitally by both a DSLR camera and a smartphone were 0.000 and 1.000 at 24 cm, 0.000 and 1.000 at 28 cm, and 0.000 and 1.000 at 32 cm (Table 1).
The means and standard deviations (SD) of the width of attached gingiva measured digitally by both a DSLR camera and a smartphone were 3.4765 ± 0.47486 and 3.4765 ± 0.47486 at 24 cm, 3.3765 ± 0.47486 and 3.3765 ± 0.47486 at 28 cm, and 3.2765 ± 0.47486 and 3.3059 ± 0.46250 at 32 cm. The t-values and P values of the width of attached gingiva measured digitally with both a DSLR camera and a smartphone were 0.000 and 1.000 at 24 cm, 0.000 and 1.000 at 28 cm, and -0.259 and 0.797 at 32 cm (Table 1).
The gingival colors assessed digitally with a DSLR camera and a smartphone at 24, 28, and 32 cm were pink (58.8%), coral pink (14.7%), and red (26.5%). There was no difference in color assessment at any of the three distances between the DSLR camera and smartphone sources (Figure 3)(Supplementary file 1).
Inter-group comparison: traditional vs. camera vs. smartphone
No statistically significant differences were observed in gingival characteristics measured by traditional clinical exam, professional camera imaging, and smartphone imaging (Supplementary file 2).
Width of KG: The mean widths measured by traditional clinical examination (5.70 ± 0.56 mm), professional camera imaging (5.73 ± 0.60 mm), and smartphone imaging (5.61 ± 0.62 mm) were very similar (P = 0.442), indicating that both imaging modalities can consistently reproduce the traditional clinical measurement of KG width (Table 2).
Height of interdental papilla (IDP): The height measurements followed a similar pattern with means of approximately 2.4–2.6 mm for all methods and no significant differences (P = 0.485). This indicates that imaging methods can determine IDP height (Table 2).
Gingival margin (GM) position: The mean GM position value was the same for camera imaging (0.47 ± 0.79) and smartphone imaging, and comparable to the standard method, with a P-value of 1.000, which indicated perfect agreement (Table 2).
Gingival color: Among the categories (pale pink, coral pink, red), the proportions of gingival color were not significantly different across the three methods used (P = 0.185). Although the proportion of pale pink gingiva was larger in the traditional method group (76.5%) than in the two imaging methods (58.8%), the difference was not statistically significant. Participants demonstrated a consistent ability to assess gingival color using both camera and smartphone imaging (Table 2 and Figure 4). Gingival color assessment in pictures captured with a camera and a smartphone was performed using the standardized CIELab color measurement method, yielding precise, standardized results (Figures 5 and 6).
Table 1.
Comparison of the mean ± SD of the width of keratinized gingiva, height of interdental papilla, gingival margin position, and width of attached gingiva at 24, 28, and 32 cm using DSLR and smartphone cameras
|
Parameter
|
Group
|
N
|
Mean (mm)
|
SD
|
t-value
|
P
value
|
| Width of keratinized gingiva (KG) at 24 cm |
DSLR camera |
34 |
5.73 |
0.60 |
0.774 |
0.442 |
| Smartphone camera |
34 |
5.61 |
0.62 |
| KG at 28 cm |
DSLR camera |
34 |
5.59 |
0.64 |
0.643 |
0.522 |
| Smartphone camera |
34 |
5.49 |
0.64 |
| KG at 32 cm |
DSLR camera |
34 |
5.43 |
0.60 |
0.215 |
0.831 |
| Smartphone camera |
34 |
5.39 |
0.64 |
| Height of interdental papilla (IDP) at 24 cm |
DSLR camera |
34 |
2.48 |
0.44 |
0.723 |
0.485 |
| Smartphone camera |
34 |
2.41 |
0.43 |
| IDP at 28 cm |
DSLR camera |
34 |
2.38 |
0.44 |
0.723 |
0.485 |
| Smartphone camera |
34 |
2.31 |
0.43 |
| IDP at 32 cm |
DSLR camera |
34 |
2.28 |
0.44 |
0.723 |
0.485 |
| Smartphone camera |
34 |
2.21 |
0.43 |
| Gingival margin (GM) position at 24 cm |
DSLR camera |
34 |
0.47 |
0.79 |
0.000 |
1.000 |
| Smartphone camera |
34 |
0.47 |
0.79 |
| GM at 28 cm |
DSLR camera |
34 |
0.47 |
0.79 |
0.000 |
1.000 |
| Smartphone camera |
34 |
0.47 |
0.79 |
| GM at 32 cm |
DSLR camera |
34 |
0.47 |
0.79 |
0.000 |
1.000 |
| Smartphone camera |
34 |
0.47 |
0.79 |
| Width of attached gingiva (AG) at 24 cm |
DSLR camera |
34 |
3.48 |
0.47 |
0.000 |
1.000 |
| Smartphone camera |
34 |
3.48 |
0.47 |
| AG at 28 cm |
DSLR camera |
34 |
3.38 |
0.47 |
0.000 |
1.000 |
| Smartphone camera |
34 |
3.38 |
0.47 |
| AG at 32 cm |
DSLR camera |
34 |
3.28 |
0.47 |
−0.259 |
0.797 |
| Smartphone camera |
34 |
3.31 |
0.46 |
KG: Keratinized gingiva; IDP: Interdental Papilla; GM: Gingival margin; AG: Attached gingiva.
The t-value quantifies how large the difference between group means is relative to sample variability, while the p-value shows the probability of observing such a difference (or a more extreme one) if the null hypothesis were true—typically, P < 0.05 indicates a statistically significant result.
Table 2.
Comparison of gingival parameter measurements using the traditional periodontal probe method (group 1), DSLR camera method (group 2), and smartphone method (group 3)
|
Parameter
|
Traditional method (n=34) Group 1
|
Camera imaging
(n=34) Group 2
|
Smartphone imaging
(n=34) Group 3
|
P
value
|
| Width of keratinized gingiva (KG) (mm) |
5.70 ± 0.56 |
5.73 ± 0.60 (at 24 cm) |
5.61 ± 0.62 (at 24 cm) |
0.442 |
| Height of interdental papilla (IDP) (mm) |
Mode = 3; Mean ≈ 2.63 |
2.48 ± 0.44 (at 24 cm) |
2.41 ± 0.43 (at 24 cm) |
0.485 |
| Gingival margin (GM) position (mm) |
Mostly 0; few cases with 1 or 2 |
0.47 ± 0.79 |
0.47 ± 0.79 |
1.000 |
| Gingival color |
26 Pale pink (76.5%) 4 Coral (11.8%) 4 Red (11.8%) |
20 Pale pink (58.8%) 5 Coral (14.7%) 9 Red (26.5%) |
20 Pale pink (58.8%) 5 Coral (14.7%) 9 Red (26.5%) |
0.185 |

Figure 1.
DSLR camera setup used for gingival imaging
.
DSLR camera setup used for gingival imaging

Figure 2.
Smartphone setup used for gingival imaging
.
Smartphone setup used for gingival imaging
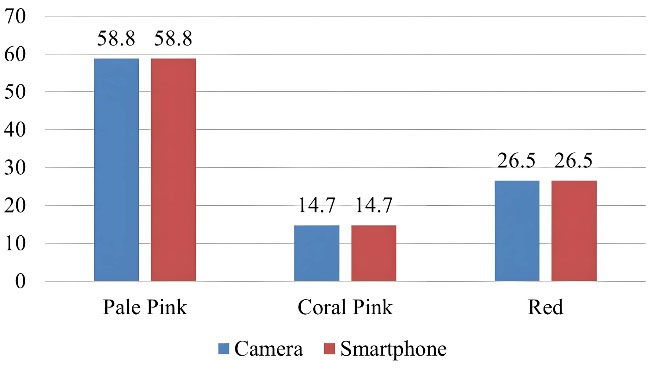
Figure 3.
Gingival color comparison between DSLR camera and smartphone at 24, 28, and 32 cm
.
Gingival color comparison between DSLR camera and smartphone at 24, 28, and 32 cm
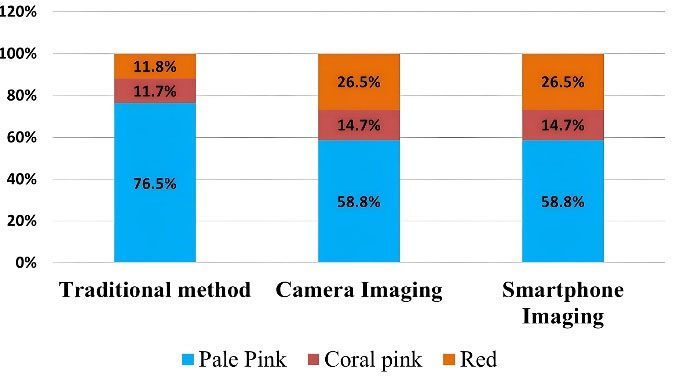
Figure 4.
Gingival color comparison between the traditional method, DSLR camera, and smartphone imaging
.
Gingival color comparison between the traditional method, DSLR camera, and smartphone imaging

Figure 5.
Gingival color assessment using a DSLR camera at different examination distances
.
Gingival color assessment using a DSLR camera at different examination distances

Figure 6.
Gingival color assessment using a smartphone at different examination distances
.
Gingival color assessment using a smartphone at different examination distances
These results show that smartphone imaging is a tool comparable to professional camera imaging and traditional clinical assessment for determining key gingival attributes such as width, height, margin position, and color. Therefore, smartphone imaging could be used as a reliable, accessible alternative method for clinical and research applications when assessing gingival characteristics.
Discussion
This study aimed to compare the accuracy and precision of smartphone imaging with DSLR photography in assessing gingival characteristics. Although initial data on smartphone vs. DSLR imaging showed potential for clinical use, evaluations aimed at a deeper understanding of the implications are warranted to integrate the data into broader clinical literature.
Technically, the assessment of focusing and distance estimation in the work of Healy and Stephan advances our understanding of smartphone vs. DSLR photography, with clearly identified limitations related to device-specific variance and experience.10 Controllers of device and user experience were clearly needed, which necessitate operational processes, calibration devices, and potentially software enhancements (i.e., AI computer-aided corrections) to ensure consistency for smartphone imaging.
Recent research demonstrated that smartphones are increasingly feasible for clinical photography, and Yung et al14 noted that new smartphone cameras can achieve color accuracy similar to that of a DSLR system in a controlled clinical setting. They recommended smartphones for intraoral photography, provided that user protocols for lighting and positioning are followed. This is consistent with our results, which showed that smartphone photography can reasonably represent gingival color and contour.
Additionally, Lazar et al15 explored the use of smartphones for aesthetic evaluation in dentistry and concluded that smartphones could be appropriately used for preliminary aesthetic evaluations, particularly in low-resource environments or for patient self-assessment. Our results endorse this use, especially for screening or follow-up purposes, although professional systems provided more detailed images with more consistent image quality across different lighting conditions.
Gingival health and color consistency were assessed following scaling and root planing using high-resolution digital imaging and precise image processing techniques. The study seeks to determine whether smartphone cameras can serve as a cost-effective, easy alternative to professional devices for diagnosing and monitoring gingival diseases in clinical settings.13-15
The use of DSLR and smartphone cameras enables a comparison of their performance in terms of color correctness, resolution, and gingival parameter evaluation. The use of ImageJ software for image analysis ensures impartiality in image analysis, providing a consistent way to measure and compare gingival health. This method is clinically relevant because it allows for non-invasive monitoring of gingival health using pre- and post-treatment photographs, allowing clinicians to track improvements in gingival color and other key parameters following scaling and root planing, assisting in the evaluation of treatment effectiveness.16,17
Moussa et al18 conducted a study to compare linear measures of clay models taken with DSLR and smartphone cameras to digital models. The measures of anterior teeth taken with DSLR and smartphone cameras (at all distances tested) and scanned showed no difference. For documentation reasons, distortion is minimal, and both camera systems can be used. Dentists can use DSLR and smartphone cameras (at a minimum distance of 24 cm) to capture smiles and provide comparable, consistent linear measurements.
Lim et al19 conducted a study to revisit the gingival dimensions in a healthy Korean population using digital scanning. According to the study’s findings, gingival dimensions obtained with an intraoral scanner followed a distribution pattern similar to those found in earlier investigations. However, the proportions appear to be affected by race and/or ethnicity, particularly in the mandibular canine and second molar. Some gingival measurements may be used to differentiate between males and females.
A thorough evaluation of the relationship between periodontal phenotype and gingival dimensions found that the mean KG height ranged between 2.75 and 5.44 mm in the thin phenotype and 5.09 mm to 6.65 mm in the thick phenotype. In the current investigation, the mean keratinized gingival widths measured by DSLR and smartphone cameras at a distance of 24 cm were 5.33 mm and 5.7 mm, respectively.20
Bhatia et al21 conducted a study to measure the entire-mouth mid-buccal breadth of attached gingiva in individuals across four distinct age groups. This study also examined differences between optical and histochemical approaches for identifying the mucogingival junction and for calculating the breadth of the attached gingiva. The study’s findings revealed that the width of attached gingiva varies in different regions of the mouth and increases with age, with no significant differences in the evaluation technique. The present study results are also consistent with this study, which employed both DSLR and smartphone cameras to examine gingival features with no significant difference in the mode of photography.
Kuppusamy et al22 conducted a study to assess the accuracy of smartphone photos for dental health screening in children compared with clinical examination. The pilot study found that a mobile teledentistry technique using smartphone photos can diagnose caries, plaque, and gingival status in children, with diagnostic accuracy comparable to that of a visual clinical examination. Compared with a visual clinical examination, smartphone cameras can be a more reliable and convenient option for screening for enamel and dentin carious lesions, dental plaque, and gingival health. The current study’s findings are also consistent with Kuppusamy et al’s22 study, which employed both DSLR and smartphone cameras to examine gingival features with no significant difference in the photographic approach.
Summary and outcome of the study
The clinical measurements, such as the width of KG, attached gingiva, interdental papilla height, gingival margin position, and gingival color, were accurate at 24 cm with both DSLR and smartphone cameras, compared with the traditional clinical measurements using a probe and color assessment by visual examination.
Using DSLR cameras and smartphones to assess clinical parameters in patients with gingivitis offers numerous benefits for documentation, diagnosis, patient involvement, and remote treatment. Nonetheless, it is important to thoroughly assess image quality, consistency, and data protection.
Despite considerable interest in developing non-invasive approaches to assess gingival health, existing research remains somewhat limited. Advancements in optical imaging, salivary biomarkers, and diverse diagnostic technologies may revolutionize the assessment of gingival health, reducing patient discomfort and enhancing the accuracy and accessibility of early disease identification.
Potential clinical impact and future research directions
This study has important clinical implications by assessing the reliability of smartphone-based imaging for objectively evaluating gingival characteristics compared with professional equipment. If smartphone-based imaging is validated. Mobile phone imaging could make oral health monitoring accessible to everyone by enabling remote, inexpensive, and cost-effective assessments of periodontal disease, particularly in disadvantaged or low-resource populations.
While using an 18–55-mm kit lens in place of a dedicated macro lens could affect the measurement accuracy and comparability of the present study relative to previous studies, dedicated macro lenses are designed to provide greater magnification with minimal distortion. Specifically, where kit lenses may introduce slight distortion and a decrease in depth of field, this may impact reproducibility. In light of these limitations, one could argue that this may exacerbate the perceived differences in the quality of professional images compared to smartphone images; therefore, the equivalence of image findings should be taken with caution.
Future studies should consider developing an imaging protocol standardized across multiple smartphone models, using color calibration devices, and developing computerized diagnostic support systems powered by artificial intelligence to increase the accuracy of the resulting images. Additionally, longitudinal studies could assess the feasibility of using mobile imaging to track disease progression or treatment outcomes in periodontal patients.
Future research might mitigate this impact by using standard external light sources, e.g., ring flashes and dual-point flashes, which provide more uniform illumination and reduce opportunities for shadows or glare on surfaces.
Limitations
This study was limited by potential variability in lighting conditions, camera resolution, and image capture angles, which may have influenced the accuracy of gingival parameter measurements. Differences in operator handling and ambient illumination could also affect image consistency between smartphone and professional camera recordings. Additionally, the study’s sample size and controlled clinical setting might not fully represent real-world conditions.
Conclusion
The present study demonstrates that non-invasive digital imaging can reliably quantify gingival clinical characteristics. Smartphone imaging produced measurements comparable to those obtained with a professional DSLR camera across key parameters, including the width of KG, the height of the interdental papilla, the position of the gingival margin, and gingival color. These findings indicate that smartphone-based imaging is a feasible and accessible alternative for assessing gingival health, particularly in settings where professional photographic equipment may not be available. Integration of digital imaging into clinical practice may enhance documentation, facilitate patient education, and support consistent follow-up evaluations.
Competing Interests
The authors declare that they have no competing interests.
Data Availability
The data are presented as supplementary files.
Ethical Approval
All the procedures were in accordance with the ethical standards of the National Committee on Human Experimentation and with the Helsinki Declaration of 1975, as revised in 2013. The study was explained to patients, and a detailed informed consent was obtained from all the participants. The study was approved by the Institutional Ethics Committee of Vishnu Dental College, Bhimavaram, Andhra Pradesh, India, with the reference number IECVDC/24/F/PI/IVV/49.
Supplementary Files
Supplementary file 1. Data obtained in the research.
(xlsx)
References
- Soheili F, Delfan N, Masoudifar N, Ebrahimni S, Moshiri B, Glogauer M. Toward digital periodontal health: recent advances and future perspectives. Bioengineering (Basel) 2024; 11(9):937. doi: 10.3390/bioengineering11090937 [Crossref] [ Google Scholar]
- Saincher R, Kumar S, Gopalkrishna P, Maithri M, Sherigar P. Comparison of color accuracy and picture quality of digital SLR, point and shoot and mobile cameras used for dental intraoral photography - a pilot study. Heliyon 2022; 8(4):e09262. doi: 10.1016/j.heliyon.2022.e09262 [Crossref] [ Google Scholar]
- Shah N, Rai J, Shah M, Gupte M. Clinical evaluation and digital photographic analysis: a modern approach to assess gingival depigmentation. World J Dent 2024; 14(12):1084-90. doi: 10.5005/jp-journals-10015-2348 [Crossref] [ Google Scholar]
- Vijyakumar M, Ashari A, Yazid F, Rani H, Kuppusamy E. Reliability of smartphone images to assess plaque score among preschool children: a pilot study. J Clin Pediatr Dent 2024; 48(2):143-8. doi: 10.22514/jocpd.2024.042 [Crossref] [ Google Scholar]
- Gangwani P, Chuang SK, Derenzi A, Aziz S. Is there a difference in quality of photographs obtained using smartphones, compared to the photographs obtained via digital single-lens reflex camera?. Oral Surg Oral Med Oral Pathol Oral Radiol 2024; 138(5):613-8. doi: 10.1016/j.oooo.2024.06.009 [Crossref] [ Google Scholar]
- Hardan LS, Moussa C. Mobile dental photography: a simple technique for documentation and communication. Quintessence Int 2020; 51(6):510-8. doi: 10.3290/j.qi.a44365 [Crossref] [ Google Scholar]
- Hardan L, Bourgi R, Cuevas-Suárez CE, Lukomska-Szymanska M, Monjarás-Ávila AJ, Zarow M. Novel trends in dental color match using different shade selection methods: a systematic review and meta-analysis. Materials (Basel) 2022; 15(2):468. doi: 10.3390/ma15020468 [Crossref] [ Google Scholar]
- Park JC, Lee JM, Kwon HJE. Moonshot thinking in periodontology. J Periodontal Implant Sci 2021; 51(2):75-6. doi: 10.5051/jpis.215102edi01 [Crossref] [ Google Scholar]
- Nalbantoğlu AM, Yanık D. Revisiting the measurement of keratinized gingiva: a cross-sectional study comparing an intraoral scanner with clinical parameters. J Periodontal Implant Sci 2023; 53(5):362-75. doi: 10.5051/jpis.2204320216 [Crossref] [ Google Scholar]
- Healy SS, Stephan CN. Focus distance estimation from photographed faces: a test of PerspectiveX using 1709 frontal and profile photographs from DSLR and smartphone cameras. Int J Legal Med 2023; 137(6):1907-20. doi: 10.1007/s00414-023-03078-y [Crossref] [ Google Scholar]
- Kalpana D, Rao SJ, Joseph JK, Kurapati SK. Digital dental photography. Indian J Dent Res 2018; 29(4):507-12. doi: 10.4103/ijdr.IJDR_396_17 [Crossref] [ Google Scholar]
- Shahrul AI, Shukor N, Norman NH. Technique for orthodontic clinical photographs using a smartphone. Int J Dent 2022; 2022:2811684. doi: 10.1155/2022/2811684 [Crossref] [ Google Scholar]
- Vaid NR, Hansa I, Bichu Y. Smartphone applications used in orthodontics: a scoping review of scholarly literature. J World Fed Orthod 2020; 9(3S):S67-73. doi: 10.1016/j.ejwf.2020.08.007 [Crossref] [ Google Scholar]
- Yung D, Tse AK, Hsung RT, Botelho MG, Pow EH, Lam WY. Comparison of the colour accuracy of a single-lens reflex camera and a smartphone camera in a clinical context. J Dent 2023; 137:104681. doi: 10.1016/j.jdent.2023.104681 [Crossref] [ Google Scholar]
- Lazar R, Culic B, Gasparik C, Lazar C, Dudea D. Evaluation of smartphone dental photography in aesthetic analysis. Br Dent J. 2021. 10.1038/s41415-021-3619-2
- Bertl K, Bertl MH, Gotfredsen K, Heimel P, Lettner S, Bertl W. Reproducibility of intraoral photography for pink and white tissue assessment - is it worth the hassle? J Prosthodont Res 2019;63(4):404-10. Reproducibility of intraoral photography for pink and white tissue assessment - is it worth the hassle? J Prosthodont Res 2019; 63(4):404-10. doi: 10.1016/j.jpor.2019.04.001 [Crossref] [ Google Scholar]
- Wee AG, Lindsey DT, Kuo S, Johnston WM. Color accuracy of commercial digital cameras for use in dentistry. Dent Mater 2006; 22(6):553-9. doi: 10.1016/j.dental.2005.05.011 [Crossref] [ Google Scholar]
- Moussa C, Hardan L, Kassis C, Bourgi R, Devoto W, Jorquera G. Moussa C, Hardan L, Kassis C, Bourgi R, Devoto W, Jorquera G, et alAccuracy of dental photography: professional vssmartphone’s camera. Biomed Res Int 2021; 2021:3910291. doi: 10.1155/2021/3910291 [Crossref] [ Google Scholar]
- Lim HC, Lee J, Kang DY, Cho IW, Shin HS, Park JC. Digital assessment of gingival dimensions of healthy periodontium. J Clin Med 2021; 10(8):1550. doi: 10.3390/jcm10081550 [Crossref] [ Google Scholar]
- Zweers J, Thomas RZ, Slot DE, Weisgold AS, Van der Weijden FG. Characteristics of periodontal biotype, its dimensions, associations and prevalence: a systematic review. J Clin Periodontol 2014; 41(10):958-71. doi: 10.1111/jcpe.12275 [Crossref] [ Google Scholar]
- Bhatia G, Kumar A, Khatri M, Bansal M, Saxena S. Assessment of the width of attached gingiva using different methods in various age groups: a clinical study. J Indian Soc Periodontol 2015; 19(2):199-202. doi: 10.4103/0972-124x.152106 [Crossref] [ Google Scholar]
- Kuppusamy E, Mohamad Nazri SN, Mohd Sultan F, Yazid F, Ashari A. The accuracy of smartphone images for oral health screening among children compared to clinical examination: a pilot study. J Health Transl Med (JUMMEC). 2024(1):258-66. doi: 10.22452/jummec.sp2024no1.25