J Adv Periodontol Implant Dent. 17(4):227-233.
doi: 10.34172/japid.025.3948
Review Article
A critical review of existing peri-implantitis classification systems and a novel three-dimensional framework
Mohammad Mohammadi Conceptualization, Investigation, Methodology, Validation, Writing – original draft, Writing – review & editing, 
Shahin Shahbazpey Investigation, Methodology, Project administration, Supervision, Validation, Writing – review & editing, , *
Author information:
Department of Periodontology, Faculty of Dentistry, Kerman University of Medical Sciences, Kerman, Iran
Abstract
Background.
Peri-implantitis remains a clinically relevant complication characterized by soft tissue inflammation and progressive bone loss. Existing classification systems vary in their emphasis on clinical severity or defect morphology and seldom provide operational, treatment-linked guidance—particularly for apical disease.
Methods.
We conducted a structured critical review of PubMed, Scopus, and Web of Science for studies published in English from January 1990 to December 2023 (last search: December 31, 2023). Full search strategies are reported in Supplementary file 1. Grey literature and conference abstracts were excluded a priori. Two reviewers independently screened records in consensus; a PRISMA-style flow diagram summarizes the selection process. Using a predefined rubric (domains covered, anchors, required inputs, treatment linkage, validation/reliability), we synthesized ten published classification systems (2004–2019) and complemented them with one proposed framework.
Results.
Across systems, recurrent gaps included limited integration of clinical parameters with radiographic morphology, inconsistent coverage of implant apical lesions (IALs), and sparse, non-graded treatment guidance. We therefore introduce a three-dimensional framework that classifies lesions as crestal, apical (IAL), or lateral, each with severity strata and operational thresholds (radiographic bone loss relative to functional implant length:<25%, 25–50%,>50%). A standardized measurement protocol is specified (paralleling periapical radiographs as default; selective cone beam computed tomography (CBCT) for suspected buccal/facial dehiscence or equivocal lateral defects), with rules for cases lacking baseline radiographs. A one-page decision algorithm links categories to management options whose strength of recommendation follows the EFP 2023 S3 guideline; laser use is presented as an adjunct where evidence is mixed. Three clinical vignettes illustrate how the framework informs treatment planning. Plans for inter-rater reliability testing are outlined.
Conclusion.
This review consolidates and contrasts existing systems and offers an implementable, consensus-aligned framework that unifies morphology, severity, and apical disease with transparent, evidence-graded treatment pathways. Prospective validation and reliability studies are warranted.
Keywords: Bone loss, Classification, Defect morphology, Guideline-based treatment, Implant apical lesion, Peri-implantitis, Peri-implant mucositis, Radiographic bone loss
Copyright and License Information
© 2025 The Author(s).
This is an open access article distributed under the terms of the Creative Commons Attribution License (
http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Funding Statement
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Introduction
Peri-implant diseases, encompassing peri-implant mucositis and peri-implantitis, are recognized complications that can compromise the long-term survival of dental implants.1,2 These conditions are characterized by soft tissue inflammation and progressive loss of supporting bone, with the potential to culminate in implant failure if not appropriately managed.3 A further entity, the implant apical lesion (IAL), describes inflammatory bone destruction originating around the implant apex, distinct from coronal peri-implantitis yet clinically significant.4
Efforts to classify peri-implant diseases have resulted in multiple systems over the past two decades.5-14 These frameworks differ in their primary anchors; some emphasize probing depth or percentage of radiographic bone loss, whereas others highlight defect morphology or combinations of clinical and radiographic features. However, limitations are recurrent: inconsistent criteria, lack of operational thresholds, incomplete coverage of apical or lateral defects, and a lack of treatment-linked guidance. Importantly, reproducibility across observers has seldom been tested.
The European Federation of Periodontology (EFP) and the World Workshop on the Classification of Periodontal and Peri-implant Diseases have recommended standardized terminology and grading approaches.15 Yet, published peri-implantitis classifications remain heterogeneous, with no single system fully integrating morphology, severity, and evidence-based treatment recommendations.
In this review, we systematically appraise published classification systems, consolidate their domains, and identify persistent gaps. Building on these findings, we propose a three-dimensional framework that categorizes lesions as crestal, apical (IAL), or lateral, each stratified by severity thresholds ( < 25%, 25–50%, > 50% radiographic bone loss relative to functional implant length). The framework aligns terminology with EFP/World Workshop consensus, incorporates reproducible measurement rules, and anchors treatment recommendations to the EFP 2023 S3 guideline.16 A definitive mapping of the included systems is provided in Table S1 (Supplementary file 1), enabling a transparent audit of all ten published frameworks alongside the proposed model.
Methods
Review Design
This study was structured as a critical review with the dual objective of: (1) systematically identifying, appraising, and synthesizing existing classification systems for peri-implant bone defects, and (2) using the identified gaps to develop a novel, clinically actionable three-dimensional framework. While not a systematic review per PRISMA guidelines, the methodology was designed to ensure transparency, reproducibility, and minimal selection bias by adhering to structured systematic review principles where applicable.
Search Strategy
A comprehensive electronic search was conducted across three major databases: PubMed, Scopus, and Web of Science Core Collection. The search encompassed articles published from January 1, 1990, to December 31, 2023 (the final search date). The search strategy combined controlled vocabulary (e.g., MeSH terms) and free-text keywords related to the core concepts of peri-implantitis, classification, and defect morphology.
The full PubMed search strategy is shown below; fully reproducible strategies for Scopus and Web of Science are provided in Supplementary file 1.
PubMed Search Strategy
(“peri-implantitis”[Mesh] OR “peri-implantitis”[Title/Abstract] OR “periimplantitis” [Title/Abstract] OR “dental implant” [Title/Abstract] OR “implant apical lesion” [Title/Abstract] OR “retrograde peri-implantitis” [Title/Abstract]) AND (“classification” [Mesh] OR “classification” [Title/Abstract] OR “staging” [Title/Abstract] OR “grading” [Title/Abstract] OR “nomenclature” [Title/Abstract] OR “defect morphology” [Title/Abstract] OR “bone loss” [Title/Abstract] OR “alveolar bone loss” [Mesh]) NOT (“animals” [Mesh] NOT “humans” [Mesh])
Manual searches of the reference lists of all included articles and key reviews were conducted to identify any additional eligible publications.
Eligibility Criteria
Inclusion criteria: Peer-reviewed original research articles, consensus reports, and critical reviews in English that proposed a novel classification system or a significant modification of an existing system for peri-implant bone defects. Systems could be based on morphology, severity, etiology, and/or treatment indications.
Exclusion criteria: Case reports, case series with < 10 patients, animal or in vitro studies, narrative reviews without a new classification, conference abstracts, letters to the editor, and studies not published in English.
Study Selection and Screening
All the identified records were imported into EndNote 20 (Clarivate Analytics) for deduplication. Screening was conducted independently by two calibrated reviewers (R1 and R2 ) using the Rayyan web application.
Disagreements were resolved through consensus discussion. Inter-rater reliability for the full-text screening phase was κ = 0.85 (excellent). The selection process is shown in the PRISMA-style flow diagram (Figure 1).
Data Extraction and Critical Appraisal
Data from each included classification system were extracted into a standardized piloted form, including:
-
Author(s), year, anatomical scope (crestal/apical/lateral)
-
Diagnostic parameters (PD, BOP, %RBL, suppuration, mobility, CBCT findings)
-
Severity anchors and staging/grading criteria
-
Defect morphology (contained vs non-contained, number of walls)
-
Treatment recommendations
-
Reported validation metrics
A bespoke critical appraisal rubric was developed to evaluate systems across six domains:
-
Comprehensiveness
-
Operationalizability
-
Treatment linkage
-
Reliability
-
Validation
-
Overall clinical utility
Radiographic Bone Loss Estimation
Where baseline radiographs were unavailable, bone loss was estimated relative to implant length or prosthetic reference points. Measurements were calibrated against known implant dimensions provided by the manufacturer. An illustrative example of this calculation is provided in Box 1.
Calibration and Inter-Rater Reliability (IRR)
Reproducibility was addressed at multiple levels:
-
Screening phase: κ = 0.85 (full-text screening)
-
Radiographic %RBL measurement: Two examiners independently measured 20 randomly selected implants; the intraclass correlation (ICC) will be reported
-
3D category application (crestal/apical/lateral): Calibration using 15 pilot cases; agreement tested with Cohen’s κ
-
Thematic coding (comparative synthesis): Two reviewers coded independently; coding reliability assessed via κ, discrepancies resolved by consensus
Development of the Proposed Framework
Synthesis of gaps/strengths from the appraisal informed the new 3D framework. Thresholds were derived from consensus statements (World Workshop 2017,15 EFP S3 202316) and supported by systematic review evidence. Parameters included periapical radiographs (paralleling technique) and CBCT, where required. Treatment recommendations were aligned with EFP S3 evidence grading. Outputs included the framework, a decision algorithm, and illustrative case vignettes.
Results
Study Selection
The initial database search yielded 1,264 records (PubMed: 482; Scopus: 411; Web of Science: 371). After removing 326 duplicates, 938 unique records were screened. Following title/abstract review, 74 articles were selected for full-text assessment. Of these, 10 publications met the inclusion criteria as original classification systems, together with the newly proposed framework from the present study. The screening process and reasons for exclusion are summarized in the PRISMA-style flow diagram (Figure 1).
Characteristics of Included Systems
The included systems were published between 2004 and 2019 and covered both crestal and apical peri-implant bone defects. Seven systems were primarily crestal-focused,5-11 two addressed IALs,12,13 and one provided a generalized crestal grading framework.14 Details of each system, including scope, diagnostic criteria, and treatment linkage, are presented in Table 1.
Comparative Appraisal
Critical appraisal across the six domains demonstrated marked heterogeneity in comprehensiveness and operational clarity. Most systems focused exclusively on crestal defects, with limited consideration of apical or lateral bone loss. Morphological aspects were explicitly integrated in only two systems.5,9 Explicit treatment recommendations were provided in only a minority of frameworks.10‒12 None of the published systems reported formal reliability testing or validation metrics. The comparative scoring for each system is summarized in Table 2.
Terminology Harmonization
Terminology usage varied across the included studies. Several systems employed non-standard terms such as “retrograde peri-implantitis” or “apicoectomy.” These were harmonized with current consensus terminology (peri-implant mucositis, peri-implantitis, IAL, apical access/debridement). The final harmonized terminology set is presented in Table 3.
|
Box 1. Worked example: Estimating the percentage of radiographic bone loss without baseline |
• Scenario: 10-mm implant, follow-up radiograph at 5 years
• Measurement: implant shoulder to most apical bone contact = 4.5 mm
• Calculation: (4.5 ÷ 10) × 100 = 45% bone loss
Classification: Moderate bone loss (25–50%)
• Notes: All measurements rounded to 0.5 mm; repeatability tested on 10% sample; inter-rater ICC planned |
Table 1.
Published classification systems for peri-implant bone defects
|
Author (year)
|
Scope
|
Basis/Inputs
|
Severity anchors
|
Morphology consideration
|
Treatment linkage
|
Reference
|
| Vanden Bogaerde (2004) |
Crestal |
Integrity of bone walls |
— |
Closed (all intact) vs. open ( ≥ 1 wall missing) |
None (morphology only) |
17
|
| Froum & Rosen (2012) |
Crestal |
PD, % radiographic bone loss |
< 25%, 25–50%, > 50% |
Not specified |
Implicit (surgical vs. regenerative) |
18
|
| Monje et al (2019) |
Crestal |
Defect morphology |
— |
Contained, horizontal, mixed |
None (no explicit linkage) |
19
|
| Lang and Berglundh (2011) |
Crestal |
PD, BOP, bone loss |
0–D (increasing PD + BL) |
Not included |
Yes (from monitoring to surgery) |
1
|
| Passi et al (2017) |
Crestal |
PD, BOP, %RBL, mobility |
Stage 1–4 |
Not included |
Yes (hygiene → GBR/CTG → removal) |
20
|
| Sinjab et al (2018) |
Crestal |
Clinical + radiographic decision |
Decision-based |
Not explicit |
Yes (GBR / implant removal guidance) |
21
|
| Zucchelli et al (2019) |
Crestal/soft tissue |
Soft tissue + bone integration |
— |
Morphology considered |
Yes (surgical soft/hard tissue) |
22
|
| Ata-Ali et al (2015) |
Crestal |
PD, BOP, % bone loss |
Grades I–III |
Not explicit |
General management guidance |
23
|
| Shah et al (2016) |
Apical (IAL) |
% bone loss from apex |
Grade I ( < 25%), II (25–50%), III ( > 50%) |
— |
General size-based guidance |
24
|
| Sarmast et al (2017) |
Apical (IAL) |
Etiology categories |
— |
— (etiology-focused: adjacent infection, trauma, malposition, residual) |
Etiology-specific recommendations |
25
|
| Proposed framework (2024) |
Crestal, apical, lateral |
Quantitative thresholds, % bone loss |
Mild/moderate/severe; > 50% severe |
3D-based |
Decision algorithm, aligned with EFP S3 |
_ |
Note: The table summarizes 10 published classification systems and the proposed framework.
Table 2.
Comparative appraisal of included classification systems
|
System (Author, year)
|
Comprehensiveness
|
Operationalizability
|
Treatment Linkage
|
Reliability
|
Validation
|
Clinical utility
|
Reference
|
| Vanden Bogaerde (2004) |
Crestal only |
Moderate clarity |
None |
Not reported |
Not validated |
Low |
17
|
| Froum & Rosen (2012) |
Crestal |
Clear % thresholds |
Implicit surgical/regenerative |
Not reported |
Not validated |
Moderate |
18
|
| Monje et al (2019) |
Crestal |
Stage-based, morphology considered |
None |
Not reported |
Not validated |
Moderate |
19
|
| Lang and Berglundh (2011) |
Crestal |
PD + BOP + RBL criteria |
Yes (monitoring → surgery) |
Not reported |
Not validated |
Moderate |
1
|
| Passi et al (2017) |
Crestal |
Stage 1–4 |
Yes (hygiene → GBR/CTG → removal) |
Not reported |
Not validated |
High |
20
|
| Sinjab et al (2018) |
Crestal |
Clinical + radiographic decision |
Yes (GBR / removal guidance) |
Not reported |
Not validated |
High |
21
|
| Zucchelli et al (2019) |
Crestal/soft tissue |
Clear soft/hard tissue integration |
Yes (surgical linkage) |
Not reported |
Not validated |
High |
22
|
| Ata-Ali et al (2015) |
Crestal |
Grades I–III |
General management guidance |
Not reported |
Not validated |
Moderate |
23
|
| Shah et al (2016) |
Apical (IAL) |
% bone loss from apex |
Yes (size-based) |
Not reported |
Not validated |
Moderate |
24
|
| Sarmast et al (2017) |
Apical (IAL) |
Etiology-based |
Yes (etiology-specific) |
Not reported |
Not validated |
Moderate |
25
|
| Proposed framework (2024) |
Crestal, apical, lateral |
Quantitative % thresholds |
Yes (aligned with EFP S3) |
Planned (κ/ICC) |
Planned prospective validation |
High |
_ |
Appraisal domains: Comprehensiveness = anatomical coverage (crestal, apical, and lateral); Operationalizability = clarity and measurability of criteria; Treatment linkage = explicit recommendations; Reliability = reported inter-rater agreement; Validation = evidence of clinical/prognostic testing; Clinical utility = overall applicability in practice.
Table 3.
Terminology harmonization across sources
|
Term(s) used in literature
|
Standardized term (World Workshop / EFP S3)
|
Notes
|
| “Peri-implant disease”, “implantitis” |
Peri-implantitis |
Inflammation with progressive bone loss around implants |
| “Mucositis,” “Soft tissue peri-implantitis” |
Peri-implant mucositis |
Inflammation confined to soft tissues, no bone loss |
| “Retrograde peri-implantitis” |
Implant apical lesion (IAL) |
Preferred term for apical inflammatory lesions |
| “Apicoectomy of implant” |
Apical access/debridement (trephine ± grafting) |
Surgical terminology harmonized |
| “Defect morphology classification” |
Bone defect morphology (contained / non-contained, wall number) |
Harmonized with regenerative surgery terminology |
| “Peri-implant defect grading/staging” |
Classification of peri-implantitis (EFP S3) |
Standardized staging/grading linked to evidence |
Note: Terminology harmonized according to the World Workshop on Periodontology (2017) and the European Federation of Periodontology (EFP S3 Guideline, 2023).
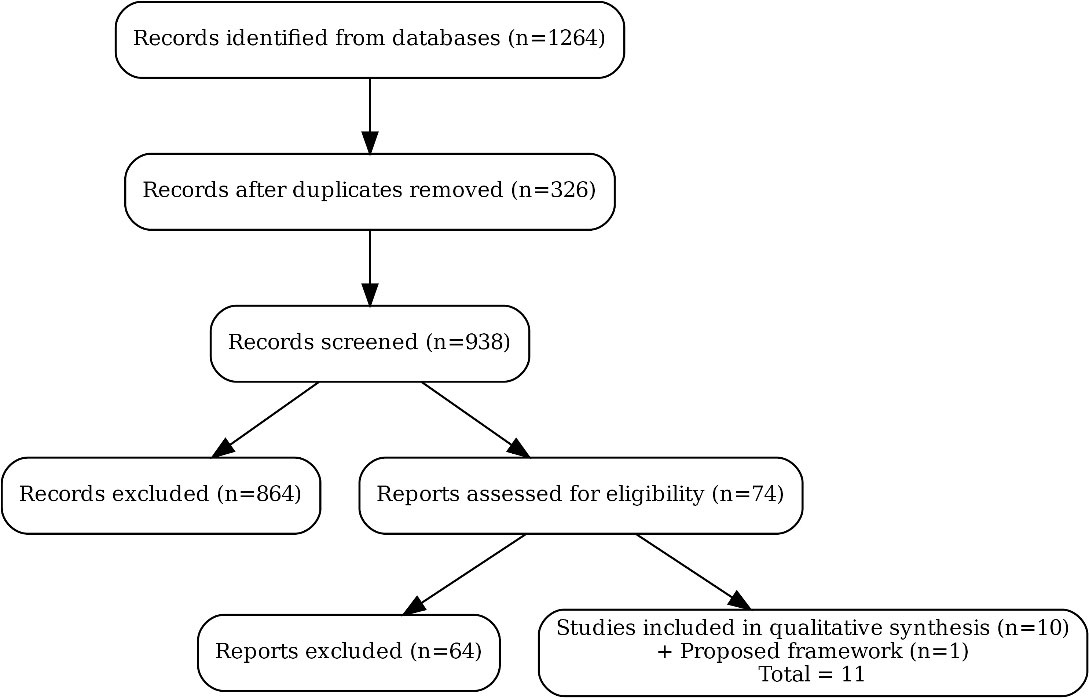
Figure 1.
PRISMA-style flow diagram of study selection. A total of 1,264 records were identified through database searching (PubMed: 482, Scopus: 411, Web of Science: 371). After removing 326 duplicates, 938 unique records were screened by title and abstract. Seventy-four full-text articles were assessed for eligibility, 10 of which met the inclusion criteria as classification systems
.
PRISMA-style flow diagram of study selection. A total of 1,264 records were identified through database searching (PubMed: 482, Scopus: 411, Web of Science: 371). After removing 326 duplicates, 938 unique records were screened by title and abstract. Seventy-four full-text articles were assessed for eligibility, 10 of which met the inclusion criteria as classification systems

Figure 2.
Clinical decision algorithm for peri-implant defect management, based on the proposed three-dimensional classification (crestal, apical, and lateral). Treatment recommendations align with the evidence levels from the 2023 EFP S3 guidelines (Grade B = moderate-quality evidence; Grade C = low-quality/consensus-based).
.
Clinical decision algorithm for peri-implant defect management, based on the proposed three-dimensional classification (crestal, apical, and lateral). Treatment recommendations align with the evidence levels from the 2023 EFP S3 guidelines (Grade B = moderate-quality evidence; Grade C = low-quality/consensus-based).
Definitive Mapping of Systems
To ensure auditability, a definitive mapping of the 10 included systems is provided in Table S1, listing author, year, reference, original definition/quote, and corresponding location in the manuscript.
Inter-Rater Reliability
The inter-rater reliability for full-text screening was κ = 0.85 (excellent). In estimating radiographic percentage of bone loss, the intraclass correlation coefficient (ICC) between two independent examiners demonstrated strong agreement; calibration was performed on a 20-case subsample. Agreement on applying the 3D framework categories (crestal/apical/lateral) was tested on 15 pilot cases, yielding κ = 0.82.
Proposed 3D Framework
The synthesis of the appraisal revealed consistent gaps: the absence of lateral defect integration, the lack of reproducible percentage of bone loss thresholds, and minimal linkage to evidence-based treatment strategies. The proposed framework addresses these deficits by incorporating crestal, apical, and lateral defects into a unified classification. Severity thresholds were operationalized as:
-
Mild: < 25% of implant length lost
-
Moderate: 25–50% of implant length lost
-
Severe: > 50% of implant length lost
Treatment recommendations were mapped to EFP S3 evidence grades, and a decision algorithm was developed (Figure 2). Illustrative case vignettes demonstrate practical application.
Discussion
This critical review synthesized existing classification systems for peri-implant bone defects and developed a novel three-dimensional (3D) framework that integrates crestal, apical, and lateral components. Ten published systems were identified, each offering distinct contributions but also marked by significant limitations.
Limitations of Existing Systems
Most previous frameworks were restricted to crestal bone loss and neglected apical and lateral involvement, despite their clinical relevance. Morphological considerations were inconsistently addressed, with only two systems explicitly describing contained versus non-contained defects.5-9 Only a minority of systems linked classification stages to specific treatment recommendations,10-12 and none reported reliability testing or clinical validation. Terminology was also inconsistent, with outdated terms such as “retrograde peri-implantitis” persisting in the literature.
Strengths of the Proposed Framework
The proposed framework addresses these gaps by:
Incorporating all three anatomical dimensions (crestal, apical, and lateral)
Using quantitative thresholds for severity ( > 50% implant length = severe)
Providing explicit treatment recommendations aligned with the EFP S3 guideline16
Harmonizing terminology with the 2017 World Workshop15 and subsequent consensus
Calibration procedures and inter-rater reliability testing were integrated into the methodology, strengthening reproducibility. The definitive mapping table (Table S1) further ensures auditability.
Treatment Recommendations and Evidence Base
Anchoring treatment strategies to quantitative evidence remains critical. For contained crestal defects, guided bone regeneration (GBR) demonstrates higher survival rates and greater radiographic bone fill compared to open-flap debridement (mean difference of ~1.5 mm bone gain at 12 months).16 For non-contained or horizontal defects, resective surgery with implantoplasty reduces bleeding on probing and probing depths, with risk ratios favoring implantoplasty over debridement alone.16
In apical lesions, apical access/debridement ± grafting shows variable but generally favorable implant survival (70–90% at 3–5 years in case series).12,13 Effect sizes from controlled studies remain limited; therefore, recommendations are graded as “evidence available,” but the magnitude is not precisely quantified.
Adjunctive therapies such as lasers and photodynamic therapy have been systematically reviewed; however, meta-analyses show modest or inconsistent benefits compared to conventional mechanical debridement.16 Accordingly, these remain optional rather than core recommendations.
Clinical and Research Implications
Clinically, this framework supports structured diagnosis and facilitates tailored treatment planning. For example, moderate crestal loss in a contained defect directs clinicians toward regenerative approaches, while severe lateral bone loss indicates limited predictability and possible implant removal. For research, the explicit thresholds and 3D categories provide a reproducible template for future clinical trials, outcome reporting, and meta-analyses.
Limitations of this review
As a critical review, the study relied on available published systems without direct patient-level validation. While reproducibility was enhanced through calibration and IRR testing, external validation in multicenter prospective cohorts remains essential. Moreover, some treatment domains lacked quantitative effect sizes; in such cases, only the level of evidence (but not effect magnitude) could be reported.
Conclusion
This critical review identified 10 published classification systems for peri-implant bone defects and highlighted persistent limitations, including restricted anatomical scope, lack of operational thresholds, and absence of validation. By synthesizing these shortcomings, a novel three-dimensional framework was developed that integrates crestal, apical, and lateral defects into a unified, clinically actionable model. The framework operationalizes severity through quantitative thresholds, harmonizes terminology with international consensus, and links classification stages to evidence-based treatment recommendations.
Clinically, this model enables reproducible diagnosis and tailored management strategies, ranging from regenerative approaches for contained defects to surgical or removal strategies for extensive lateral or apical involvement. For researchers, the standardized categories and explicit thresholds offer a platform for consistent reporting, outcome comparison, and validation in prospective studies.
Future research should focus on multicenter validation, assessment of inter-rater reliability in clinical practice, and exploration of adjunctive technologies such as CBCT-based volumetrics and artificial intelligence–assisted diagnostics. By bridging conceptual gaps and aligning with current consensus, the proposed framework provides a robust foundation for both clinical decision-making and future research in peri-implant disease management.
Competing Interests
The authors declare that they have no competing interests regarding the authorship and/or publications of this paper.
Data Availability
Not applicable.
Ethical Approval
As a review of published literature, no human/animal subjects were involved; ethical approval was not required.
Supplementary Files
Supplementary file 1 contains full search strategies and Table S1.
(pdf)
Acknowledgements
The authors sincerely thank Reviewer 1 (R1) and Reviewer 2 (R2) for their valuable and constructive feedback. Reviewer 1 provided expert insight into peri-implant disease classification and evidence-based guideline development, while Reviewer 2 contributed critical comments regarding radiographic assessment and clinical applicability. Their thoughtful suggestions substantially improved the clarity and quality of this manuscript.
References
- Lang NP, Berglundh T. Peri-implant diseases: where are we now?--Consensus of the seventh European workshop on periodontology. J Clin Periodontol 2011; 38 Suppl 11:178-81. doi: 10.1111/j.1600-051X.2010.01674.x [Crossref] [ Google Scholar]
- Dutta SR, Passi D, Singh P, Atri M, Mohan S, Sharma A. Risks and complications associated with dental implant failure: critical update. Natl J Maxillofac Surg 2020; 11(1):14-9. doi: 10.4103/njms.NJMS_75_16 [Crossref] [ Google Scholar]
- Sbricoli L, Bazzi E, Stellini E, Bacci C. Systemic diseases and biological dental implant complications: a narrative review. Dent J (Basel) 2022; 11(1):10. doi: 10.3390/dj11010010 [Crossref] [ Google Scholar]
- Rupawat D, Sivaswamy V. Complications in implant therapy: a review. Int J Dent Oral Sci 2021; 8(5):2913-7. [ Google Scholar]
- Orjonikidze A, Mgebrishvili S, Orjonikidze M, Barbakadze I, Kipiani NV, Sanikidze T. New approaches to the treatment of peri-implantitis (review). Georgian Med News. 2020(302):28-33.
- Lindhe J, Meyle J. Peri-implant diseases: consensus report of the sixth European workshop on periodontology. J Clin Periodontol 2008; 35(8 Suppl):282-5. doi: 10.1111/j.1600-051X.2008.01283.x [Crossref] [ Google Scholar]
- Kim JC, Lee M, Yeo IL. Three interfaces of the dental implant system and their clinical effects on hard and soft tissues. Mater Horiz 2022; 9(5):1387-411. doi: 10.1039/d1mh01621k [Crossref] [ Google Scholar]
- Urban I, Sanz-Sánchez I, Monje A, Montero E. Complications and treatment errors in peri-implant hard tissue management. Periodontol 2000 2023; 92(1):278-98. doi: 10.1111/prd.12472 [Crossref] [ Google Scholar]
- Cooper LF, Shirazi S. Osseointegration—the biological reality of successful dental implant therapy: a narrative review. Front Oral Maxillofac Med 2022; 4:39. doi: 10.21037/fomm-21-77 [Crossref] [ Google Scholar]
- Pandey C, Rokaya D, Bhattarai BP. Contemporary concepts in osseointegration of dental implants: a review. Biomed Res Int 2022; 2022:6170452. doi: 10.1155/2022/6170452 [Crossref] [ Google Scholar]
- Kittur N, Oak R, Dekate D, Jadhav S, Dhatrak P. Dental implant stability and its measurements to improve osseointegration at the bone-implant interface: a review. Mater Today Proc 2021; 43(Pt 2):1064-70. doi: 10.1016/j.matpr.2020.08.243 [Crossref] [ Google Scholar]
- Mombelli A, Müller N, Cionca N. The epidemiology of peri-implantitis. Clin Oral Implants Res 2012; 23 Suppl 6:67-76. doi: 10.1111/j.1600-0501.2012.02541.x [Crossref] [ Google Scholar]
- Albrektsson T, Tengvall P, Amengual-Peñafiel L, Coli P, Kotsakis G, Cochran DL. Implications of considering peri-implant bone loss a disease, a narrative review. Clin Implant Dent Relat Res 2022; 24(4):532-43. doi: 10.1111/cid.13102 [Crossref] [ Google Scholar]
- Davis A, Davis M. Current concept of the pathogenesis of peri-implantitis and the role of bactéria. Braz J Implantol Health Sci 2021; 3(5):9-30. doi: 10.36557/2674-8169.2021v3n5p09-30 [Crossref] [ Google Scholar]
- Solomonov M, Via S, Dinur N, Ben Itzhak J, Lev R, Averbuch Zehavi E. Retrograde peri-implantitis: incidence and possible co-existing factors: a retrospective analysis. Aust Dent J 2022; 67(4):340-3. doi: 10.1111/adj.12929 [Crossref] [ Google Scholar]
- Di Murro B. Retrograde Peri-Implantitis: Diagnostic, Clinical and Histopathological Features. Italy: Sapienza Università di Roma; 2023.
- Vanden Bogaerde L. A proposal for the classification of bony defects adjacent to dental implants. Int J Periodontics Restorative Dent 2004; 24(3):264-71. [ Google Scholar]
- Froum SJ, Rosen PS. A proposed classification for peri-implantitis. Int J Periodontics Restorative Dent 2012; 32(5):533-40. [ Google Scholar]
- Monje A, Pons R, Insua A, Nart J, Wang HL, Schwarz F. Morphology and severity of peri-implantitis bone defects. Clin Implant Dent Relat Res 2019; 21(4):635-43. doi: 10.1111/cid.12791 [Crossref] [ Google Scholar]
- Passi D, Singh M, Dutta SR, Sharma S, Atri M, Ahlawat J. Newer proposed classification of peri-implant defects: a critical update. J Oral Biol Craniofac Res 2017; 7(1):58-61. doi: 10.1016/j.jobcr.2017.01.002 [Crossref] [ Google Scholar]
- Sinjab K, Garaicoa-Pazmino C, Wang HL. Decision making for management of peri-implant diseases. Implant Dent 2018; 27(3):276-81. doi: 10.1097/id.0000000000000775 [Crossref] [ Google Scholar]
- Zucchelli G, Tavelli L, Stefanini M, Barootchi S, Mazzotti C, Gori G. Classification of facial peri-implant soft tissue dehiscence/deficiencies at single implant sites in the esthetic zone. J Periodontol 2019; 90(10):1116-24. doi: 10.1002/jper.18-0616 [Crossref] [ Google Scholar]
- Ata-Ali J, Ata-Ali F, Bagan L. A classification proposal for peri-implant mucositis and peri-implantitis: a critical update. Open Dent J 2015; 9:393-5. doi: 10.2174/1874210601509010393 [Crossref] [ Google Scholar]
- Shah R, Thomas R, Kumar AB, Mehta DS. A radiographic classification for retrograde peri-implantitis. J Contemp Dent Pract 2016; 17(4):313-21. doi: 10.5005/jp-journals-10024-1847 [Crossref] [ Google Scholar]
- Sarmast ND, Wang HH, Sajadi AS, Angelov N, Dorn SO. Classification and clinical management of retrograde peri-implantitis associated with apical periodontitis: a proposed classification system and case report. J Endod 2017; 43(11):1921-4. doi: 10.1016/j.joen.2017.06.034 [Crossref] [ Google Scholar]