J Adv Periodontol Implant Dent. 17(4):216-226.
doi: 10.34172/japid.025.3827
Review Article
In-situ gel drug delivery system as a viable approach to periodontal therapy: A comprehensive review
Supreeth Sirangala Vivek Conceptualization, Data curation, Investigation, Methodology, Visualization, Writing – original draft, Writing – review & editing, 
Venkatesh Dinnekere Puttegowda Data curation, Formal analysis, Investigation, Methodology, Project administration, Supervision, Validation, Visualization, Writing – review & editing, , *
Joysa Ruby Joseph Rajarathinam Data curation, Methodology, Project administration, Validation, Visualization, Writing – review & editing,
Gunashekar Dhanapal Resources, Writing – review & editing,
Naveen Kumar Karimaranahalli Banappa Resources, Writing – review & editing,
Chaithanya Kadalu Mahendra Resources, Writing – review & editing,
Pooja Rangadham Resources, Writing – review & editing,
Author information:
Department of Pharmaceutics, Acharya & BM Reddy College of Pharmacy Soldevanahalli, Hesaraghatta Road, Bengaluru-560107 Karnataka, India
Abstract
This narrative review summarizes recent advances in in situ gel drug delivery systems for periodontal therapy, focusing on formulation strategies, the pharmaceutical agents involved, and their clinical applications. A comprehensive search was conducted on PubMed, Scopus, and Google Scholar for English-language articles published from 2000 to 2024 using relevant keywords. Articles were selected based on their clinical significance, scientific rigor, and relevance to periodontal treatment. In situ gels use physiological stimuli such as pH, temperature, or ions for sol-to-gel transition, enabling sustained and localized drug release into periodontal pockets. These systems aim to improve therapeutic efficacy and reduce systemic side effects. However, limitations like inconsistent gelation, low mechanical strength, and limited long-term clinical data hinder widespread clinical adoption. Future research should focus on formulation optimization and rigorous clinical trials to facilitate the integration of in-situ gels into routine periodontal care.
Keywords: Antibiotics, Carbopol, Controlled drug delivery, In situ gel, Periodontal disease
Copyright and License Information
© 2025 The Author(s).
This is an open access article distributed under the terms of the Creative Commons Attribution License (
http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Funding Statement
No specific grant was obtained from any funding organization: public, private, or non-profit for this study.
Introduction
Periodontitis is a complex, chronic, inflammatory disease caused by biofilms. Multiple factors contribute to the damage of the periodontal apparatus. Understanding the role of bacteria in periodontal disease is crucial for prevention and treatment.1 Loss of tissue attachment, loss of alveolar bone, and formation of pockets are the primary signs of periodontal disease symptoms. Clinical studies have shown that scaling and root planing, along with the removal of bacterial deposits from the tooth surface, effectively reduce probing pocket depths. Antimicrobial strategies have been developed and tested to eliminate all microorganisms associated with periodontal disease since mechanical debridement alone is insufficient for this purpose.2 Hundreds of different types of anaerobic and aerobic bacteria make up the oral microbiota. Deep-layer microorganisms adhere to and are compactly arranged against the tooth, while more motile forms inhabit the superficial layers. Biofilms refer to the growth on tooth surfaces in the form of complex mixed colonies that exist interdependently.3 The most common microorganisms causing periodontal disease are Gram-negative anaerobic bacilli, including many anaerobic spirochetes and some anaerobic cocci. Porphyromonas gingivalis, Bacteroides forsythus, Prevotella intermedia, Actinobacillus actinomycetemcomitans, and Treponema denticola are the main microorganisms associated with severe periodontal lesions.4 The goals of modern periodontitis treatment are to reduce infection, decrease inflammation, and establish a clinical state consistent with periodontal health. The first line of treatment for periodontitis is usually non-surgical, encompassing scaling and root planing (SRP) alongside oral hygiene instructions.5 In the treatment of periodontitis, systemic antibiotics should not be used alone. Systemic antibiotics are effective antibacterial agents for treating periodontal diseases when used in conjunction with adequate mechanical debridement to disrupt subgingival biofilms. The best antibiotic, dosage, duration, and timing are all subjects of debate. In cases where aggressive periodontitis is present, adjunctive systemic antibiotics should be considered. Although data indicate that supplemental systemic antibiotics provide additional therapeutic benefits in treating persistent periodontitis in deep pockets, the decision to prescribe antibiotics should be made on an individual basis.6,7 The rise in antibiotic resistance began to be acknowledged in the 1980s. The medical profession has overlooked the fact that microorganisms have been using antibiotics to combat each other for over two billion years, and during these decades of arrogance, they have developed resistance mechanisms to overcome them. Antibiotics will never fully “defeat” bacteria. The resistance is unavoidable.8 Non-steroidal anti-inflammatory drugs (NSAIDs) are among the most commonly used medications worldwide. They are prescribed to treat fever, inflammation, and pain. The term “NSAID” can apply to a broad category of medications used to manage chronic rheumatic conditions related to periodontitis.9,10
An in situ gel system with a local anesthetic is preferable to an emulsion-based drug delivery system, as it is easy to apply to the periodontal pocket, remains at the application site for the required duration, provides a quick onset of anesthesia that lasts throughout the dental procedure, and can be easily rinsed out with water afterward. Topical formulations for local anesthetics in periodontal pockets are rare, but in situ gel systems have garnered significant interest from pharmaceutical developers as a drug delivery vehicle for dermal, nasal, ocular, oral, buccal, vaginal, rectal, and parenteral administration.11 The advantages of in situ polymer delivery systems include ease of drug delivery, decreased administration rates, controlled release, improved patient tolerance, and convenience; they are also biocompatible and biodegradable, fostering interest in these formulations.12 Additionally, the formulation is simpler, which lowers manufacturing costs and investments.13 There are three types of in situ gelling systems: ion-activated systems like gellan gum and sodium alginate; temperature-dependent systems such as Pluronic and polymethacrylates; and pH-triggered systems like carbopol and cellulose acetate phthalate.14,15 This local medication therapy raises the question of whether to use it as an adjunctive technique to scaling and root planing or as a definitive treatment alternative. There are several reasons to avoid using local medication delivery systems as an alternative technique: Patients with adult periodontitis treated by scaling and/or root planing achieve equivalent clinical outcomes compared to those who received drug therapy alone, which also avoids introducing the risk of drug-resistant bacterial strains; root planing can help disrupt and eliminate biofilms that are less likely to respond to local drug delivery; root surface instrumentation can remove calculus, which may contain endotoxins that inhibit plaque accumulation; and scaling and root planing in maintenance patients may be less costly when applied to all affected teeth.16 Periodontal treatment often employs locally applied antibiotics like tetracycline, doxycycline, metronidazole, and minocycline due to their antimicrobial action against both Gram-positive and Gram-negative organisms. As tetracycline analogs, doxycycline and minocycline have enhanced lipid solubility and longer action, while metronidazole effectively combats anaerobic infections. Table 1 presents the critical features of these antibiotics.1
Methods
An extensive search of PubMed, Scopus, and Google Scholar was performed until March 2024, with the keywords “in situ gel” or “gel-forming system” in combination with “periodontal disease” or “periodontitis” or “periodontal therapy” with “drug delivery” or “mucoadhesive” or “local delivery.” A manual search from the bibliographies of the selected articles and relevant reviews was also performed.
The areas of interest for the review included:
-
Which in situ gel-based drug delivery systems have been developed for periodontal therapy?
-
On what formulation bases, mechanisms of action, and clinical effectiveness have they been reported?
Articles eligible for inclusion discussed in situ gel systems for localized drug delivery, specifically in periodontal treatment. Only articles in English with full-text availability were included. Exclusion criteria included studies involving routes other than periodontal (such as ophthalmic, nasal, etc.), gels not classified as drugs, animal or in vitro studies with no clinical correlation, abstracts without full data, as well as patent applications and editorials without experimental proof.
Titles and abstracts were screened first. Full texts were assessed if they met the inclusion criteria or if their abstracts were considered unclear. Both authors independently assessed all studies that were finally included. The extracted data consisted of formulation compositions, type of gel system (thermoresponsive, ion-sensitive, pH-sensitive), active pharmaceutical ingredients, polymer characteristics, route of administration, drug release profile, and any clinical findings.
Results
A total of 1,126 articles were retrieved from PubMed, Scopus, and Google Scholar. The titles, abstracts, and full texts were screened against the inclusion and exclusion criteria, leading to a final total of 42 articles selected for the review. The selected studies were segregated and systematically discussed under six themes: thermoresponsive in situ gels, ion-sensitive gels, pH-responsive systems, mucoadhesive and polymer-based formulations, drugs commonly incorporated in periodontal gels, and clinical evaluation of their therapeutic effectiveness. These categories greatly helped in organizing the findings related to formulation design, gelation triggers, drug release profile, and periodontal outcome systematically.
Periodontal disease
Periodontal disease is a chronic inflammatory condition characterized by the formation of periodontal pockets, gingival inflammation, loss of connective tissue attachment, and eventual tooth loss.17,18 The traditional definition of periodontal disease refers to the progressive degeneration of the hard and soft tissues of the periodontal complex, caused by dysbiotic bacterial colonies coexisting symbiotically with aberrant immune responses in the gingiva and periodontal tissues.19
The progression of periodontal disease from healthy gingiva to advanced periodontitis is characterized by increasing pocket depths, alveolar bone loss, and inflammation (Figure 1).
Etiopathogenesis of periodontal diseases
Since Anton von Leeuwenhoek’s report of the presence of “animalcules” in dental plaque, it has been understood that these bacteria are present in the oral cavity. For over a century, the bacterial etiology of periodontal disorders has been studied and developed with technological advancements in characterization and identification.20
The etiopathogenesis of periodontal diseases involves a complex relationship between microbial populations. Early colonizers such as Gemella, Atopobium, Fusobacterium nucleatum, Streptococcus sanguis, S. mitis, and Capnocytophaga species inhabit healthy periodontal tissues, most beneficial to the host.21,22 Gingivitis occurs with both Gram-negative (Campylobacter gracilis, F. nucleatum, Prevotella intermedia, andVeillonella) and Gram-positive (Streptococcus spp., Actinomyces viscosus, andPeptostreptococcus micros) species, the former being particularly characteristic in pregnancy-related gingivitis.22-24 Chronic periodontitis, however, is marked by increased levels of pathogens like Tannerella forsythia, Campylobacter rectus, P. intermedia, Porphyromonas gingivalis, and F. nucleatum.22-25 Localized aggressive periodontitis (LAP) is the focus of Actinobacillus actinomycetemcomitans, withEikenella corrodens, P. gingivalis, and C. rectus.26,27 The microbiological picture of generalized aggressive periodontitis is similar to that of chronic periodontitis because of similar etiologies.28 Necrotizing ulcerative gingivitis is most commonly linked with spirochetes and fusobacteria, such as the newly discovered Treponema putidum.29 Periodontal abscesses include the presence of bacteria such as T. forsythia, C. rectus, P. gingivalis, F. nucleatum, P. intermedia, and P. micros.30
Classification
To facilitate more accurate diagnosis and treatment of periodontal and peri-implant diseases, the 2017 American Academy of Periodontology (AAP/EFP) and European Federation of Periodontology classification incorporated staging, grading, and more categories. Practitioners can use this new paradigm to assist in diagnosis, treatment planning, and long-term follow-up. Table 2 outlines the classification.31,32
Periodontitis clinical signs
Gingival inflammation, pocket formation, bone loss, clinical attachment loss, tooth mobility, and foul breath, all of which are recognized symptoms of periodontitis. Some of these symptoms include gingival redness, swelling, and tenderness; gingival bleeding; receding gingiva; chronic bad breath; pain or discomfort; changes in occlusion; and pus formation between the teeth and gingiva. As periodontitis progresses, increased tooth mobility, root surface exposure, and the formation of periodontal abscesses may occur. Other symptoms consist of bleeding gums, gingival recession, chronic bad breath, soreness or discomfort, changes in occlusal alignment, and pus formation between the gums and teeth.33,34
Risk factors for periodontal disease
A vast array of risk factors contribute to the development of periodontal disease. Over half of the instances are brought about by smoking, a factor also linked to cancer and oral ulcers.35,36 While more studies are required to fully appreciate the contribution of nutrition, poor diet and vitamin C deficiency can exacerbate periodontal diseases.37 Beyond its contribution to advanced periodontitis, excessive consumption of alcohol is often concomitant with smoking and poor diet.38,39 Through physiological mechanisms, stress is involved in susceptibility to periodontal disease.40,41Additionally, genetics is also involved, as certain inherited characteristics affect dental and gingival health.42,43
Treatment
Medications are used to enhance the results and encourage recovery from periodontitis. There are regenerative agents such as bone morphogenetic protein-7 (BMP-7) and zinc-hydroxyapatite nanoparticles, and antibiotics such as levofloxacin, minocycline, tetracycline, ornidazole, metronidazole, and doxycycline that are effective in treating periodontal disease.44 Nonsteroidal anti-inflammatory drugs used to treat periodontal diseases are aspirin, flurbiprofen, ibuprofen, naproxen, piroxicam, diclofenac sodium, meloxicam, nimesulide, etodolac, and celecoxib.45For periodontal treatment, several local sustained drug delivery systems have been developed; these can be broadly classified generically as reservoir and matrix types. Depending on the use, these are made up of fibers, films, injectables, microcapsules, and gels/ointments, which incorporate both biodegradable and non-biodegradable components. Table 3 summarizes the categories and materials used in these systems.46
In situ gel systems
In situ gel administration is a good method of treating periodontitis because it continuously and carefully administers medication to the infected location. Researchers used ingredients such as zein, borneol, piperine, and curcumin to develop a formulation that targeted the inflammatory state linked to dysbiosis in periodontitis, thus showing antibacterial properties.34 To deliver these gels in a liquid state that turns into a gel when it comes into contact with the target site, so that there can be sustained drug release and better therapeutic results.34-47
In situ gels comprise hydroxy propyl methyl cellulose (HPMC), sodium alginate, and xanthan gum; these polymers improve the viscosity and control the rates of drug release. These systems have been used to produce in situ gel for administration routes such as ocular, oral, and nasal for the treatment of ulcer diseases, eye infections, rheumatoid arthritis, and so on.48
Using in situ gel involves administering the formulation in a microsyringe and directly introducing it into the periodontal pocket, where it undergoes sol-to-gel transition at the infected site (Figure 2).
Formulation
Selection of a vehicle
The right vehicle must be selected before the in situ gelling system can be prepared. Polymer dispersions were thus prepared in several buffer solutions, among which were phosphate-buffered IP (pH = 6.0), citrophosphate-buffered IP (pH = 5.0, 6.0), and acetate-buffered IP (pH = 4.0, 5.0).49
pH-induced system
All the sensitive polymers to pH contain either basic or acidic groups, which, depending on the pH of their surroundings, release or accept a proton. Gel swelling is directly proportional to the increase in external pH when anionic groups are present; otherwise, it decreases when cationic groups are present in the polymer. It comprises in situ gel from a variety of pH-sensitive polymers, such as carbopol; the physiological shift in pH has caused the solution-gel transition.50
In situ gel systems activated by temperature
Before they harden inside the targeted tissue, organ, or body cavity, these injectable solutions can be given minimally invasively. A temperature-activated solution is used in mucoadhesive formulations to gel transition polymer over a temperature range of 25–37 °C. Polymers with a low critical solution temperature of roughly 32 °C undergo a phase change at body temperature. Poloxamer is one of the numerous thermosensitive polymers that can be applied to in situ gel systems.51
The ion-activated mechanism
Gelation is triggered by a change in the ionic strength of the implanted solution. The osmotic gradient surrounding the gel surface regulates the rate of gelation. Gelation is triggered by a change in the implanted fluid’s ionic strength. The pace of gelation is regulated by the osmotic gradient surrounding the gel surface. Electrolytes such as Ca2 +, Mg2 +, and Na + cations, which are present in fluids available in the oral cavity, are crucial in the initiation of gelling when body cavities are used to deliver solutions. Alginates, hyaluronic acid, gellan gum, and gelrite are a few examples of polymers.52
Preparation of in situ gel
In situ gel is prepared by the cold method. A measured amount of polymer is slowly added to water inside a beaker with constant stirring using a magnetic stirrer. Throughout the process, the temperature of the water is maintained at 4 °C. This solution is refrigerated overnight. The preservative is dissolved in hot water to prepare the solution. After cooling, it is mixed with the above dispersion. The weighed amount of medication is dissolved in the solvents. The medication solution is mixed with the polymer dispersion as described earlier.53
Characterization
The following parameters are used to analyze and characterize the in situ gel:
Clarity
A white and black background could be used to visually review the solution and assess its clarity.54,55
Texture analysis
Using a texture profile analyzer, the gel’s consistency, stiffness, and cohesiveness are measured in situ. This mainly shows the strength of the gel and the ease of its administration in vivo; a higher adhesiveness rating is necessary to maintain close contact with the mucus surface.56
pH of gel
The pH can be found by placing the formulation in a beaker, adding 1 mL of NaOH drop by drop at a time, and constantly stirring. To check pH, a pH meter is used.57
Rheological studies
Cone and plate viscometers and Brookfield viscometers are used for viscosity. The sample tube of the in situ gel composition is filled. The viscosity of the formulation should be between 5 and 1000 mPas before gelling, and it will be between 5050,000 and 500,000 mPas (millipascal-second) once the periodontal pocket activates the ion gel.58
Swelling studies
A cell, which has been fitted with a thermal jacket to hold the temperature at a relatively constant level, is used for swelling investigations.59 Synthetic gingival crevicular fluid54 is available within the cell. One milliliter of the conditioned solution is placed in the dialysis bag, and the latter is submerged in the swelling medium. The latter is equilibrated at 370ºC. At predetermined time intervals, the bag is removed from the medium and its weight is measured. The swelling of the polymer gel as a function of time is computed and measured using the following relationship.60
%St = 100/W0 (Wt - Wo)
where St represents the swelling at the time “t,” Wo is the initial weight of the gel, and Wt is the gel’s final weight.
High-performance liquid chromatography
Reversed-phase mode is applied with the HPLC system. For analysis, a C18 Nova pack, a packed column of length (150 × 3.9 mm id), is used.61
Fourier transformer infra-red
FTIR studies explore whether drugs interact with excipients or not. KBR pellets are employed to register FTIR graphs of both the pure drugs and combinations of drugs with excipients.62
In vitro drug release studies
An in vitro release investigation of an in situ gel solution is conducted using the Franz diffusion cell. The formulation is put in the donor compartment, and freshly made gingival crevicular fluid is placed in the receptor compartment. The donor and receptor compartments are separated by the dialysis membrane, which has a hole size of 0.22 μm. A magnetic stirrer with a thermostat is used to set up the entire device. The temperature of the medium is kept at 37 ± 0.5 °C. Then, 1 mL of the sample that is removed at predetermined intervals of one hour is replaced every 6 hours with a sample volume of fresh medium. The extracted sample is diluted to 10 mL in a volumetric flask with the proper solvent using a reagent blank, and then it is analyzed by a UV spectrophotometer at the proper wavelength. An equation based on the standard calibration curve is used to determine the drug content. The cumulative drug release (CDR) percentage is calculated. For drug release data, curve fitting is performed on the gathered data. The kinetics of Fickian and Korsmeyer-Peppas diffusion mechanisms are examined using the best-fit model.54
Antimicrobial activity
Antimicrobial effectiveness experiments are performed to determine the biological activity of the sol-gel system against bacteria. This is identified using the “cup plate technique” in an agar diffusion medium. The bacterial microbial growth is tested by serial dilution of the microbiological assay compared with known concentrations of standard antibiotic preparation.54
Accelerated stability studies
According to the International Conference of Harmonization State Guidelines, the preparation is filled into amber-colored vials and closed with aluminum foil for the short-term accelerated stability study at 40 ± 20°C and 75 ± 5% RH. The sample is checked monthly for in vitro dissolution, rheological evaluation, drug content, clarity, pH, and gelling capacity.63
Commonly used polymers in the formulation of in situ gel
In situ gels are increasingly becoming renowned for their therapeutic potential in periodontal disease because they can release medication locally to the site of action in a controlled manner. Various polymers are used to form in situ gels, each of which contributes its characteristics to enhance drug delivery and therapy. The most commonly used polymers for preparing in situ gels for periodontal disease treatment are temperature-sensitive poloxamer 407, ion-sensitive gellan gum, and pH-sensitive carbopol 934P. These polymers enhance the drug’s local action and retention.64
Various polymers, including chitosan, Poloxamer 407, and sodium alginate, are used to formulate in situ gels for periodontal therapy due to their different functions, ranging from controlled drug release, mucoadhesion, and biocompatibility. Each polymer possesses its distinct advantages and disadvantages, and this could influence the effective performance of the formulations (Table 4).
Limitations of in situ gel systems
Despite its advantages, in situ gel systems have several limitations, such as insufficient mechanical strength, poor drug loading, poor gelation, and short residence times at the site of application. Precipitation of drug, sensitivity to the environment, limited release control, and stability concerns are additional challenges. To resolve these issues, strategies such as using bio-adhesive polymers, advanced encapsulation technology, and optimization of polymer formulations have been proposed. Table 5 is an overview of these limitations and potential remedies.
Efficacy of antibiotics and NSAIDs
A study thoroughly investigated the efficacy of NSAIDs and antibiotics in the treatment of periodontal disease, with significant advantages shown when combined with SRP or as part of cutting-edge delivery systems, such as in situ gels.
Antibiotics in periodontal therapy
Role: Antibiotics reduce the microbial load within periodontal pockets by specifically targeting bacteria involved in periodontal diseases, likePorphyromonas gingivalis and Aggregatibacter actinomycetemcomitans.4 Some of the antibiotics include azithromycin, doxycycline, and ornidazole.7
Clinical evidence: Systemic antibiotics and scaling and root planing significantly reduced probing pocket depths and the clinical attachment loss in comparison to the latter alone, based on a report by Herrera et al.78 Local delivery methods, including gels releasing chlorhexidine or doxycycline elevate medication levels in periodontal pockets without many systemic adverse effects.79
Effectiveness: Isolated application of antibiotics will increase clinical attachment loss and lower probing pocket depths while reducing microbial burden and inflammation.80
NSAIDs in periodontal therapy
They are also known as non-steroidal anti-inflammatory medicines.
Role: They work by inhibiting the cyclooxygenase enzymes COX-1 and COX-2, thereby reducing prostaglandin synthesis and modulating periodontal inflammation. Naproxen, ibuprofen, and diclofenac are just a few of these.15
Clinical evidence: Tonetti et al. demonstrated that systemic NSAIDs, including flurbiprofen, resulted in reduced alveolar bone loss during six months in patients with long-term periodontitis.81 Administration of NSAIDs via biodegradable gels locally decreased gastrointestinal side effects without causing tissue damage due to inflammation.82
Effectiveness: There is a significant reduction in the effects of NSAIDs on tissue edema, gingival inflammation, and matrix metalloproteinase-8 (MMP-8) and receptor activator of nuclear factor-kappa-B ligand (RANKL), which are indicators of bone resorption.83
Combination therapy
Synergistic benefits: By targeting both inflammatory pathways and microbiological etiology, NSAIDs combined with antibiotics have demonstrated cumulative benefits. Studies have shown that when treatment is compared as a combination rather than as monotherapy, a greater reduction in PPD and better gingival health status are observed.84
Clinical applications: Combining antibiotics and NSAIDs in local in situ gel systems allows for sustained release, resulting in increased absorption and decreased systemic side effects.85
Clinical evidence supporting in situ gel therapy in periodontitis
Increasing numbers of clinical trials have evaluated the efficacy of in situ gel systems for topical periodontal treatment in recent years. The devices are engineered to release antibacterial or anti-inflammatory agents directly into periodontal pockets for a protracted period to enhance clinical outcomes and patient compliance.
An in situ gel incorporating ornidazole-loaded microspheres was used in patients with chronic periodontitis in a separate clinical study. Enhanced microbiological and clinical outcomes were achieved through the great rheological properties of the formulation and long-term release of antibacterial activity.48
Based on the review, the application of locally applied antimicrobials, including doxycycline and chlorhexidine gels, as well as scaling and root planing, resulted in fewer systemic side effects and a slight but statistically significant benefit regarding clinical attachment gain and pocket depth reduction.78
When formulated as a gel and used locally, minocycline HCl microspheres significantly reduced the levels of Porphyromonas gingivalis, Tannerella forsythia, and other red-complex bacteria. Compared to SRP alone, clinical parameters like clinical attachment level (CAL) and probing pocket depth (PPD) exhibited statistically significant improvements.79
Several in vivo studies have demonstrated that many in situ gels can help improve probing pocket depth and clinical attachment level, as well as enhance antimicrobial capacity for periodontal interventions. This additional evidence suggests the use of drug gels, such as those containing minocycline, chlorhexidine, doxycycline, and ornidazole, as an adjunct to more conventional practice (Table 6).48,78,79
Table 1.
An overview of locally delivered antibiotics used in periodontitis patients
|
Locally delivered antibiotic types
|
Description
|
| Tetracycline |
Drugs within a wide range of bacteriostatic activity that act against both Gram-negative and Gram-positive bacteria. |
| Doxycycline |
A long-acting second-generation tetracycline antibiotic. |
| Metronidazole |
This chemotherapy drug is effective against both Gram-positive and Gram-negative anaerobic bacteria. |
| Minocycline |
The most lipid-soluble and potent semi-synthetic tetracycline antibiotic acts on Gram-negative and Gram-positive bacteria, including those with and without cell walls. |
Table 2.
Classification of periodontal disease
|
Category
|
Subcategories
|
| 1. Periodontal health & gingival diseases |
- Clinical health on intact periodontium
- Clinical health of the reduced periodontium
- Gingivitis: Biofilm-induced or non-biofilm-induced |
| 2. Periodontitis |
- Unified diagnosis: Periodontitis
- Staging (I–IV): Based on severity and complexity
- Grading (A–C): Based on risk factors and progression rate |
| 3. Necrotizing periodontal diseases |
- Necrotizing gingivitis
- Necrotizing periodontitis
- Necrotizing stomatitis |
| 4. Periodontitis as a manifestation of systemic diseases |
- Associated with genetic disorders or systemic diseases (Papillon–Lefèvre syndrome, hematologic disorders) |
| 5. Other conditions affecting the periodontium |
- Systemic diseases affecting periodontal tissues
- Mucogingival deformities
- Occlusal trauma
- Tooth/prosthesis-related factors |
| 6. Peri-Implant diseases and conditions |
- Peri-implant health
- Peri-implant mucositis
- Peri-implantitis
- Tissue deficiencies around implants |
Table 3.
Systems for local sustained delivery (LSDS )
|
Type
|
Sub-Type
|
Material
|
| 1] Reservoir type |
Fiber |
Non-biodegradable |
| 2] Matrix type |
Films |
Bio-degradable |
|
|
|
Non-biodegradable |
|
|
Injectable |
Thermosensitive polymers |
|
|
Microcapsule |
Gelatin, Chitosan microspheres |
|
|
Fiber |
Bio-degradable |
|
|
|
Non-biodegradable |
|
|
Gel/Ointment |
Carbopol, Chitosan, Poloxamer |
Table 4.
Polymers used in the formulation of in situ gels
|
Polymer
|
Action
|
Merits
|
Demerits
|
| Chitosan34-65 |
Mucoadhesive and antibacterial; forms a gel in response to pH |
Biocompatible, promotes wound healing, and has good mucoadhesion |
pH-sensitive gelation may vary in different oral environments |
| Pluronic F12766,67 |
Thermoresponsive gelation at body temperature |
Easy administration, suitable for sustained drug release |
Weak mechanical strength, rapid dissolution in saliva |
| Poloxamer 40766-68 |
Thermosensitive polymer; gels at physiological temperature |
Reversible gelation, biocompatible, suitable for injectable formulations |
Low mucoadhesion alone often needs a combination with mucoadhesive polymers |
| Sodium Alginate68 |
Forms gel in the presence of calcium ions (ion-sensitive) |
Biocompatible, non-toxic, forms stable gels |
Limited mechanical strength, brittle in dry conditions |
| Carbopol 934P65-69 |
Swells in water to form a gel; used for viscosity modulation |
Good control over drug release enhances adhesion |
Can irritate if used in high concentration |
| Hydroxypropyl Methylcellulose (HPMC)65-70 |
Swells upon hydration, forms a viscous gel |
Sustained drug release improves viscosity |
Limited responsiveness to external stimuli (e.g., temperature or pH) |
| Gellan Gum70 |
Ion-sensitive polymer, gels in the presence of cations |
Good mucoadhesive properties, clear gel formulation |
Requires precise ionic balance for proper gelation |
Table 5.
Limitations of in-situ gel systems
|
Limitations
|
Methods to Overcome
|
| Low mechanical strength71 |
Incorporate bio-adhesive polymers (e.g., chitosan, Carbopol) to improve strength and retention. |
| Poor drug loading efficiency72 |
Use advanced encapsulation techniques like liposomes, nanoparticles, or micelles. |
| Inconsistent gelation time73 |
Optimize polymer concentration and crosslinking agents for consistent gel formation. |
| Short retention time at application site74 |
Employ mucoadhesive agents to prolong contact duration. |
| Limited drug release control75 |
Implement dual polymer systems or controlled-release microcarriers. |
| Environmental sensitivity (pH/temperature variations)76 |
Develop stimuli-responsive gels with optimized transition points. |
| Stability issues77 |
Use stabilizers or antioxidants to improve shelf life. |
Table 6.
Summary of clinical evidence
|
Study
|
Drug/Formulation
|
Design
|
Findings
|
| Diasa et al, 2016.48 |
Ornidazole microsphere gel |
Clinical evaluation |
Sustained drug release; improved antimicrobial profile |
| Herrera et al, 2002.78 |
Chlorhexidine/doxycycline gels |
Systematic review |
Adjunctive benefit with scaling and root planing; improved clinical attachment level (CAL) and probing pocket depth (PPD) |
| Goodson et al, 2007.79 |
Minocycline gel |
Randomized controlled trial |
Reduced red-complex bacteria; improved probing pocket depth and clinical attachment level |
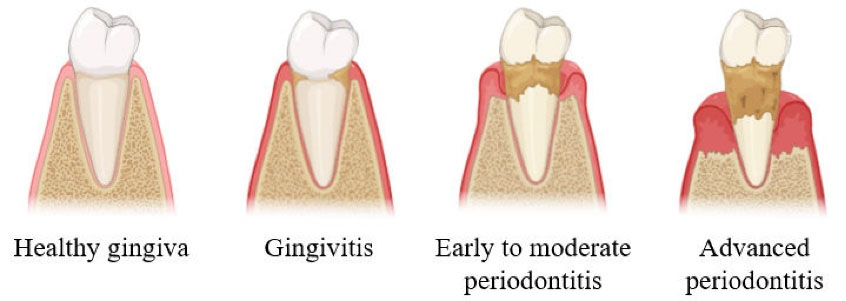
Figure 1.
Progression of periodontal disease: The stages of periodontal disease through which clinically infected periodontal tissue goes, starting with a healthy gingiva, progressing through a stage of gingivitis, and ending with periodontitis3
.
Progression of periodontal disease: The stages of periodontal disease through which clinically infected periodontal tissue goes, starting with a healthy gingiva, progressing through a stage of gingivitis, and ending with periodontitis3
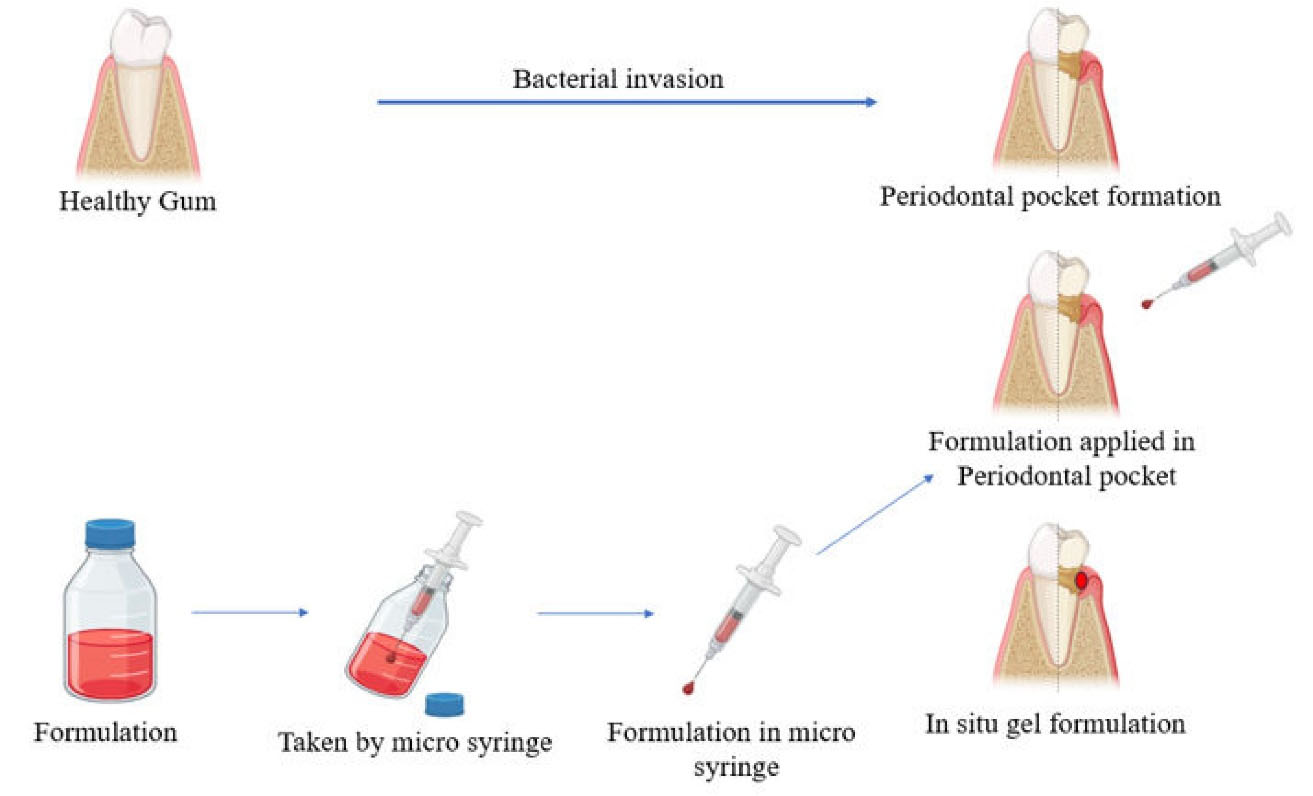
Figure 2.
Administration of in situ gel: the formulation is inserted directly into the periodontal pocket and undergoes a sol-to-gel transition at the site14
.
Administration of in situ gel: the formulation is inserted directly into the periodontal pocket and undergoes a sol-to-gel transition at the site14
Future perspectives
To improve the efficacy and delivery of NSAIDs and antibiotics in periodontal therapy, researchers have been working to develop innovative technologies, such as nanocarriers, liposomes, and biopolymer-based in situ gels.86,87
Research gap
Seemingly great from their promise to locally deliver therapeutic agents to periodontal pockets, significant gaps exist in long-term clinical validation, formulation standardization, and real-world applicability. Bridging these gaps through high-quality clinical trials and patient-centered studies is crucial for enabling their successful implementation in the clinic.
Discussion
In situ gel systems represent a promising innovation in periodontal therapy that allows for localized and sustained delivery of the drug directly into periodontal pockets. Compared to systemic treatments, these therapeutic gels enhance the therapeutic efficacy at the site of action while minimizing the systemic side effects, making them promising candidates to treat localized disease states like periodontitis. In situ gel sol-gel transition can be triggered by physiological stimuli such as pH, temperature, or ions, and hence create conditions for better retention and longer contact of the drug. Among the polymers contributing to gelation, drug release, and mucoadhesion are Poloxamer 407 (temperature-sensitive), Gellan gum (ion-sensitive), and carbopol 934P (pH-sensitive). Other polymers, like sodium alginate and chitosan, offer benefits such as biocompatibility and antibacterial activity. Since these polymers have characteristics unique to themselves that impact formulation performance, they must be chosen or combined carefully to obtain the optimum formulation. Simultaneous delivery of an antimicrobial agent (e.g., metronidazole, doxycycline) with an anti-inflammatory agent (e.g., diclofenac sodium) has a dual benefit of reducing microbiologic burden and inflammation. In line with the 2017 AAP/EFP classification emphasizing individualization of treatment,in situ gels favor customization according to factors such as disease severity, risk of progression, and patient-specific issues. However, there are formulation challenges of low mechanical strength, low drug loading, and inconsistency of gelation. Research and development in polymer science on mucoadhesive agents, nanoparticles, and dual-responsive systems are already addressing these challenges.
Therefore, in situ gels are intelligent and low-intervention methods for periodontal drug delivery. With increased research and clinical validation, they can emerge as a standard addition to the armamentarium of contemporary periodontics.
Conclusion
In situ gel-based drug delivery systems are revolutionizing the treatment of periodontal disease. They allow for localized, sustained, and controlled release of medication right in the periodontal pocket. Unlike traditional treatments, they deliver antibiotics and NSAIDs precisely where needed while keeping widespread exposure to a minimum. The mix of biocompatible polymers, innovative drug carriers, and advanced gelation methods opens up exciting possibilities for managing periodontitis effectively. However, we still need more clinical trials and advancements in formulation to make the most of this technology and get it into wider use. By incorporating responsive polymers and user-friendly designs, in situ gel technique could change periodontal therapy, providing a minimally invasive, cost-effective, and highly efficient treatment for millions affected by periodontal disease.
Competing Interests
The authors declare no personal, professional, or financial conflicts of interest that might influence the content of this paper.
Data Availability
No new data were created or analyzed in this study. Data sharing does not apply to this article as it is based solely on reviewing and analyzing previously published literature.
Ethical Approval
Since this review article does not involve human subjects, animal research, or clinical trials, ethical approval and informed consent are not needed. All information in this work arises from previously published research that has been properly referenced and credited.
Acknowledgements
The authors are thankful to the principle and management of Acharya & BM Reddy College of Pharmacy for providing facilities, including plagiarism, internet access, etc.
References
- Abu-Ta’a M, Bazzar S. Enhancing periodontitis treatment: a comprehensive literature review of locally delivered antibiotics as an adjunctive therapy. Open Dent J 2023; 17(1):e187421062308060. doi: 10.2174/18742106-v17-230809-2023-34 [Crossref] [ Google Scholar]
- Mombelli A. Microbial colonization of the periodontal pocket and its significance for periodontal therapy. Periodontol 2000 2018; 76(1):85-96. doi: 10.1111/prd.12147 [Crossref] [ Google Scholar]
- Pihlstrom BL, Michalowicz BS, Johnson NW. Periodontal diseases. Lancet 2005; 366(9499):1809-20. doi: 10.1016/s0140-6736(05)67728-8 [Crossref] [ Google Scholar]
- Kinane DF. Causation and pathogenesis of periodontal disease. Periodontol 2000 2001; 25:8-20. doi: 10.1034/j.1600-0757.2001.22250102.x [Crossref] [ Google Scholar]
- Keestra JA, Grosjean I, Coucke W, Quirynen M, Teughels W. Non-surgical periodontal therapy with systemic antibiotics in patients with untreated chronic periodontitis: a systematic review and meta-analysis. J Periodontal Res 2015; 50(3):294-314. doi: 10.1111/jre.12221 [Crossref] [ Google Scholar]
- Heitz-Mayfield LJ. Systemic antibiotics in periodontal therapy. Aust Dent J 2009; 54 Suppl 1:S96-101. doi: 10.1111/j.1834-7819.2009.01147.x [Crossref] [ Google Scholar]
- Slots J, Rams TE. Antibiotics in periodontal therapy: advantages and disadvantages. J Clin Periodontol 1990; 17(7 Pt 2):479-93. doi: 10.1111/j.1365-2710.1992.tb01220.x [Crossref] [ Google Scholar]
- Spellberg B. The future of antibiotics. Crit Care 2014; 18(3):228. doi: 10.1186/cc13948 [Crossref] [ Google Scholar]
- Moore N, Duong M, Gulmez SE, Blin P, Droz C. Pharmacoepidemiology of non-steroidal anti-inflammatory drugs. Therapie 2019; 74(2):271-7. doi: 10.1016/j.therap.2018.11.002 [Crossref] [ Google Scholar]
- Ren J, Fok MR, Zhang Y, Han B, Lin Y. The role of non-steroidal anti-inflammatory drugs as adjuncts to periodontal treatment and in periodontal regeneration. J Transl Med 2023; 21(1):149. doi: 10.1186/s12967-023-03990-2 [Crossref] [ Google Scholar]
- Kulkarni AP, Aslam Khan SK, Dehghan MH. Evaluation of polaxomer-based in situ gelling system of articaine as a drug delivery system for anesthetizing periodontal pockets–an in vitro study. Indian J Dent 2012; 3(4):201-8. doi: 10.1016/j.ijd.2012.07.006 [Crossref] [ Google Scholar]
- Bashir R, Maqbool M, Ara I, Zehravi M. An insight into novel drug delivery system: in situ gels. Cell Med 2021; 11(1):30-6. doi: 10.5667/CellMed.2021.0006 [Crossref] [ Google Scholar]
- Chaudhary B, Verma S. Preparation and evaluation of novel in situ gels containing acyclovir for the treatment of oral herpes simplex virus infections. ScientificWorldJournal 2014; 2014:280928. doi: 10.1155/2014/280928 [Crossref] [ Google Scholar]
- Al-Dabbagh AR, Alfahad M, Hameed ZA. In-situ gelling system: a promising delivery method for treating periodontitis. Iraqi J Pharm 2024; 21(3):89-101. doi: 10.33899/iraqij.p.2024.147513.1090 [Crossref] [ Google Scholar]
- Laddha UD, Mahajan HS, Patel RC. An insight to ocular in situ gelling systems. Int J Adv Pharm 2017; 6(2):31-40. doi: 10.7439/ijap.v6i2.3806 [Crossref] [ Google Scholar]
- Greenstein G, Polson A. The role of local drug delivery in the management of periodontal diseases: a comprehensive review. J Periodontol 1998; 69(5):507-20. doi: 10.1902/jop.1998.69.5.507 [Crossref] [ Google Scholar]
- Pindobilowo Pindobilowo, Tjiptoningsih UG, Ariani D. Effective tooth brushing techniques based on periodontal tissue conditions: a narrative review. Formos J Appl Sci 2023; 2(7):1649-62. doi: 10.55927/fjas.v2i7.4838 [Crossref] [ Google Scholar]
- Williams RC. Periodontal disease. N Engl J Med 1990; 322(6):373-82. doi: 10.1056/nejm199002083220606 [Crossref] [ Google Scholar]
- Sedghi LM, Bacino M, Kapila YL. Periodontal disease: the good, the bad, and the unknown. Front Cell Infect Microbiol 2021; 11:766944. doi: 10.3389/fcimb.2021.766944 [Crossref] [ Google Scholar]
- Loesche WJ, Grossman NS. Periodontal disease as a specific, albeit chronic, infection: diagnosis and treatment. Clin Microbiol Rev 2001; 14(4):727-52. doi: 10.1128/cmr.14.4.727-752.2001 [Crossref] [ Google Scholar]
- Socransky SS, Haffajee AD. The bacterial etiology of destructive periodontal disease: current concepts. J Periodontol 1992; 63(4 Suppl):322-31. doi: 10.1902/jop.1992.63.4s.322 [Crossref] [ Google Scholar]
- Tatakis DN, Kumar PS. Etiology and pathogenesis of periodontal diseases. Dent Clin North Am 2005; 49(3):491-516. doi: 10.1016/j.cden.2005.03.001 [Crossref] [ Google Scholar]
- Theilade E, Wright WH, Jensen SB, Löe H. A longitudinal clinical and bacteriological investigation. J Periodontal Res 1966; 1:1-13. doi: 10.1111/j.1600-0765.1966.tb01842.x [Crossref] [ Google Scholar]
- Kornman KS, Loesche WJ. The subgingival microbial flora during pregnancy. J Periodontal Res 1980; 15(2):111-22. doi: 10.1111/j.1600-0765.1980.tb00265.x [Crossref] [ Google Scholar]
- Dzink JL, Gibbons RJ, Childs WC 3rd, Socransky SS. The predominant cultivable microbiota of crevicular epithelial cells. Oral Microbiol Immunol 1989; 4(1):1-5. doi: 10.1111/j.1399-302x.1989.tb00398.x [Crossref] [ Google Scholar]
- Zambon JJ. Actinobacillusactinomycetemcomitans in adult periodontitis. J Periodontol 1994; 65(9):892-3. doi: 10.1902/jop.1994.65.9.892 [Crossref] [ Google Scholar]
- Kornman KS, Robertson PB. Clinical and microbiological evaluation of therapy for juvenile periodontitis. J Periodontol 1985; 56(8):443-6. doi: 10.1902/jop.1985.56.8.443 [Crossref] [ Google Scholar]
- Kamma JJ, Nakou M, Gmür R, Baehni PC. Microbiological profile of early onset/aggressive periodontitis patients. Oral Microbiol Immunol 2004; 19(5):314-21. doi: 10.1111/j.1399-302x.2004.00161.x [Crossref] [ Google Scholar]
- Wyss C, Moter A, Choi BK, Dewhirst FE, Xue Y, Schüpbach P. Treponemaputidum sp. nov., a medium-sized proteolytic spirochaete isolated from lesions of human periodontitis and acute necrotizing ulcerative gingivitis. Int J Syst Evol Microbiol 2004; 54(Pt 4):1117-22. doi: 10.1099/ijs.0.02806-0 [Crossref] [ Google Scholar]
- Newman MG, Sims TN. The predominant cultivable microbiota of the periodontal abscess. J Periodontol 1979; 50(7):350-4. doi: 10.1902/jop.1979.50.7.350 [Crossref] [ Google Scholar]
- Dietrich T, Ower P, Tank M, West NX, Walter C, Needleman I. Periodontal diagnosis in the context of the 2017 classification system of periodontal diseases and conditions - implementation in clinical practice. Br Dent J 2019; 226(1):16-22. doi: 10.1038/sj.bdj.2019.3 [Crossref] [ Google Scholar]
- Highfield J. Diagnosis and classification of periodontal disease. Aust Dent J 2009; 54 Suppl 1:S11-26. doi: 10.1111/j.1834-7819.2009.01140.x [Crossref] [ Google Scholar]
- Salvi GE, Lang NP. The effects of non-steroidal anti-inflammatory drugs (selective and non-selective) on the treatment of periodontal diseases. Curr Pharm Des 2005; 11(14):1757-69. doi: 10.2174/1381612053764878 [Crossref] [ Google Scholar]
- Mallamma T, Rehman SA, Goudanavar P, Akondi BR. In situ gels for periodontitis: an overview. Asian J Pharm Res Health Care 2024; 16(3):245-52. doi: 10.4103/ajprhc.ajprhc_86_24 [Crossref] [ Google Scholar]
- Peto R, Lopez AD, Boreham J, Thun M, Heath C Jr, Doll R. Mortality from smoking worldwide. Br Med Bull 1996; 52(1):12-21. doi: 10.1093/oxfordjournals.bmb.a011519 [Crossref] [ Google Scholar]
- Gelskey SC. Cigarette smoking and periodontitis: methodology to assess the strength of evidence in support of a causal association. Community Dent Oral Epidemiol 1999; 27(1):16-24. doi: 10.1111/j.1600-0528.1999.tb01987.x [Crossref] [ Google Scholar]
- Moynihan P, Petersen PE. Diet, nutrition and the prevention of dental diseases. Public Health Nutr 2004; 7(1a):201-26. doi: 10.1079/phn2003589 [Crossref] [ Google Scholar]
- Tezal M, Grossi SG, Ho AW, Genco RJ. The effect of alcohol consumption on periodontal disease. J Periodontol 2001; 72(2):183-9. doi: 10.1902/jop.2001.72.2.183 [Crossref] [ Google Scholar]
- Petersen PE, Ogawa H. Strengthening the prevention of periodontal disease: the WHO approach. J Periodontol 2005; 76(12):2187-93. doi: 10.1902/jop.2005.76.12.2187 [Crossref] [ Google Scholar]
- Genco RJ, Ho AW, Grossi SG, Dunford RG, Tedesco LA. Relationship of stress, distress and inadequate coping behaviors to periodontal disease. J Periodontol 1999; 70(7):711-23. doi: 10.1902/jop.1999.70.7.711 [Crossref] [ Google Scholar]
- Kune S. Stressful life events and cancer. Epidemiology 1993; 4(5):395-7. doi: 10.1097/00001648-199309000-00003 [Crossref] [ Google Scholar]
- Croucher R, Marcenes WS, Torres MC, Hughes F, Sheiham A. The relationship between life-events and periodontitis. A case-control study. J Clin Periodontol 1997; 24(1):39-43. doi: 10.1111/j.1600-051x.1997.tb01182.x [Crossref] [ Google Scholar]
- Genco RJ, Borgnakke WS. Risk factors for periodontal disease. Periodontol 2000 2013; 62(1):59-94. doi: 10.1111/j.1600-0757.2012.00457.x [Crossref] [ Google Scholar]
- Zheleznaya AP, Zhelezny PA, Nikolskaya MV. Use of allogeneic canned osteoplastic drugs for the treatment of chronic periodontitis. Russ J Dent 2021; 25(4):337-43. doi: 10.17816/1728-2802-2021-25-4-337-343 [Crossref] [ Google Scholar]
- Heasman PA, Hughes FJ. Drugs, medications and periodontal disease. Br Dent J 2014; 217(8):411-9. doi: 10.1038/sj.bdj.2014.905 [Crossref] [ Google Scholar]
- Sapra P, Patel BD, Patel DV, Borkhataria CH. Recent advances in periodontal formulations. Int J Pharm Chem Anal 2014; 1(1):65-74. [ Google Scholar]
- Manigauha A, Yadav S. Formulation and characterization of novel ophthalmic in situ gel of flucytosine for improved bioavailability. Pharm Biosci J 2022; 10(1):1-8. doi: 10.20510/10.20510/pbj/10/i1/1646 [Crossref] [ Google Scholar]
- Diasa RJ, Havaldara VD, Ghorpadea VS, Malia KK, Gaikwadb VK, Kumbhara DM. Development and evaluation of in-situ gel containing ornidazole loaded microspheres for treatment of periodontitis. J Appl Pharm Sci 2016; 6(10):200-9. doi: 10.7324/japs.2016.601028 [Crossref] [ Google Scholar]
- Mandal S, Thimmasetty MK, Prabhushankar G, Geetha M. Formulation and evaluation of an in-situ gel-forming ophthalmic formulation of moxifloxacin hydrochloride. Int J Pharm Investig 2012; 2(2):78-82. doi: 10.4103/2230-973x.100042 [Crossref] [ Google Scholar]
- Bajpai V. In-situ gel nasal drug delivery system-a review. Int J Pharma Sci 2014; 4(3):577-80. [ Google Scholar]
- Carone M, Spalinger MR, Gaultney RA, Mezzenga R, Hlavačková K, Mookhoek A. Temperature-triggered in situ forming lipid mesophase gel for local treatment of ulcerative colitis. Nat Commun 2023; 14(1):3489. doi: 10.1038/s41467-023-39013-3 [Crossref] [ Google Scholar]
- Mohan EC, Kandukuri JM, Allenki V. Preparation and evaluation of in-situ-gels for ocular drug delivery. J Pharm Res 2009; 2(6):1089-94. [ Google Scholar]
- Yadav R, Kanwar IL, Haider T, Pandey V, Gour V, Soni V. In situ gel drug delivery system for periodontitis: an insight review. Futur J Pharm Sci 2020; 6(1):33. doi: 10.1186/s43094-020-00053-x [Crossref] [ Google Scholar]
- Ahmed MG, Acharya A, Chaudhari R, Panicker K, Reddy R. Formulation and evaluation of in situ gel containing rosuvastatin in the treatment of periodontal diseases. J Pharm Res 2015; 14(2):45-50. doi: 10.18579/jpcrkc/2015/14/2/79082 [Crossref] [ Google Scholar]
- Katakam M, Ravis WR, Banga AK. Controlled release of human growth hormone in rats following parenteral administration of poloxamer gels. J Control Release 1997; 49(1):21-6. doi: 10.1016/s0168-3659(97)01648-9 [Crossref] [ Google Scholar]
- Jeong B, Bae YH, Lee DS, Kim SW. Biodegradable block copolymers as injectable drug-delivery systems. Nature 1997; 388(6645):860-2. doi: 10.1038/42218 [Crossref] [ Google Scholar]
- Cao SL, Ren XW, Zhang QZ, Chen E, Xu F, Chen J. In situ gel based on gellan gum as new carrier for nasal administration of mometasone furoate. Int J Pharm 2009; 365(1-2):109-15. doi: 10.1016/j.ijpharm.2008.08.042 [Crossref] [ Google Scholar]
- Bilensoy E, Rouf MA, Vural I, Sen M, Hincal AA. Mucoadhesive, thermosensitive, prolonged-release vaginal gel for clotrimazole:beta-cyclodextrin complex. AAPS PharmSciTech 2006; 7(2):E38. doi: 10.1208/pt070238 [Crossref] [ Google Scholar]
- Bhowmik M, Das S, Chattopadhyay D, Ghosh LK. Study of thermo-sensitive in-situ gels for ocular delivery. Sci Pharm 2011; 79(2):351-8. doi: 10.3797/scipharm.1010-04 [Crossref] [ Google Scholar]
- Rathore KS. In situ gelling ophthalmic drug delivery system: an overview. Int J Pharm Pharm Sci 2010; 2(4):30-4. [ Google Scholar]
- Charoo NA, Kohli K, Ali A. Preparation of in situ-forming ophthalmic gels of ciprofloxacin hydrochloride for the treatment of bacterial conjunctivitis: in vitro and in vivo studies. J Pharm Sci 2003; 92(2):407-13. doi: 10.1002/jps.10290 [Crossref] [ Google Scholar]
- Hiremath SS, Dasankoppa FS, Nadaf A, Jamakandi VG, Mulla JS, Sholapur HN. Formulation and evaluation of a novel in situ gum based ophthalmic drug delivery system of linezolid. Sci Pharm 2008; 76(3):515-32. doi: 10.3797/scipharm.0803-17 [Crossref] [ Google Scholar]
- Jain SP, Shah SP, Rajadhyaksha NS, Singh PSP, Amin PD. In situ ophthalmic gel of ciprofloxacin hydrochloride for once a day sustained delivery. Drug Dev Ind Pharm 2008; 34(4):445-52. doi: 10.1080/03639040701831710 [Crossref] [ Google Scholar]
- Swain GP, Patel S, Gandhi J, Shah P. Development of moxifloxacin hydrochloride loaded in-situ gel for the treatment of periodontitis: in-vitro drug release study and antibacterial activity. J Oral Biol Craniofac Res 2019; 9(3):190-200. doi: 10.1016/j.jobcr.2019.04.001 [Crossref] [ Google Scholar]
- El-Nablaway M, Rashed F, Taher ES, Atia GA, Foda T, Mohammed NA. Bioactive injectable mucoadhesive thermosensitive natural polymeric hydrogels for oral bone and periodontal regeneration. Front Bioeng Biotechnol 2024; 12:1384326. doi: 10.3389/fbioe.2024.1384326 [Crossref] [ Google Scholar]
- Nasra MM, Khiri HM, Hazzah HA, Abdallah OY. Formulation, in-vitro characterization and clinical evaluation of curcumin in-situ gel for treatment of periodontitis. Drug Deliv 2017; 24(1):133-42. doi: 10.1080/10717544.2016.1233591 [Crossref] [ Google Scholar]
- Brambilla E, Locarno S, Gallo S, Orsini F, Pini C, Farronato M. Poloxamer-based hydrogel as drug delivery system: how polymeric excipients influence the chemical-physical properties. Polymers (Basel) 2022; 14(17):3624. doi: 10.3390/polym14173624 [Crossref] [ Google Scholar]
- Zheng P, Liu X, Jiao Y, Mao X, Zong Z, Jia Q. Preparation and evaluation of poloxamer/carbopol in-situ gel loaded with quercetin: in-vitro drug release and cell viability study. Tissue Eng Regen Med 2024; 21(8):1153-71. doi: 10.1007/s13770-024-00671-z [Crossref] [ Google Scholar]
- Thammasut W, Rojviriya C, Chaiya P, Phaechamud T, Limsitthichaikoon S. Moxifloxacin HCl loaded-cellulose acetate butylate in situ forming gel for periodontitis treatment. AAPS PharmSciTech 2024; 25(7):242. doi: 10.1208/s12249-024-02960-1 [Crossref] [ Google Scholar]
- Thammasut W, Senarat S, Tuntarawongsa S, Narakornwit W, Rojviriya C, Pichayakorn W. Development of benzydamine HCl loaded-cellulose acetate butyrate in situ forming gels for periodontal treatment. J Drug Deliv Sci Technol 2024; 101(Pt A):106147. doi: 10.1016/j.jddst.2024.106147 [Crossref] [ Google Scholar]
- Gupta S, Archana Archana, Niranjan AK. A comprehensive review on in-situ gel drug delivery system. J Drug Deliv Ther 2022; 12(4-S):245-8. doi: 10.22270/jddt.v12i4-s.5539 [Crossref] [ Google Scholar]
- Sharma S, Sarkar G, Srestha B, Chattopadhyay D, Bhowmik M. In-situ fast gelling formulation for oral sustained drug delivery of paracetamol to dysphagic patients. Int J Biol Macromol 2019; 134:864-8. doi: 10.1016/j.ijbiomac.2019.05.092 [Crossref] [ Google Scholar]
- Agrawal M, Saraf S, Saraf S, Dubey SK, Puri A, Gupta U. Stimuli-responsive in situ gelling system for nose-to-brain drug delivery. J Control Release 2020; 327:235-65. doi: 10.1016/j.jconrel.2020.07.044 [Crossref] [ Google Scholar]
- Singh A, Kurkure S, Anardi S. Formulation and evaluation of in-situ gelling system for sustained release ophthalmic drug delivery of ciprofloxacin. World J Pharm Res 2020;9(8). 10.20959/wjpr20208-18075
- Vigani B, Rossi S, Sandri G, Bonferoni MC, Caramella CM, Ferrari F. Recent advances in the development of in situ gelling drug delivery systems for non-parenteral administration routes. Pharmaceutics 2020; 12(9):859. doi: 10.3390/pharmaceutics12090859 [Crossref] [ Google Scholar]
- Mohanty D, Bakshi V, Simharaju N, Haque MA, Sahoo CK. A review on in situ gel: a novel drug delivery system. Int J Pharm Sci Rev Res 2018; 50(1):175-81. [ Google Scholar]
- Paul S, Majumdar S, Chakraborty M. Revolutionizing ocular drug delivery: recent advancements in in situ gel technology. Bull Natl Res Cent 2023; 47(1):154. doi: 10.1186/s42269-023-01123-9 [Crossref] [ Google Scholar]
- Herrera D, Sanz M, Jepsen S, Needleman I, Roldán S. A systematic review on the effect of systemic antimicrobials as an adjunct to scaling and root planing in periodontitis patients. J Clin Periodontol 2002; 29 Suppl 3:136-59. doi: 10.1034/j.1600-051x.29.s3.8.x [Crossref] [ Google Scholar]
- Goodson JM, Gunsolley JC, Grossi SG, Bland PS, Otomo-Corgel J, Doherty F. Minocycline HCl microspheres reduce red-complex bacteria in periodontal disease therapy. J Periodontol 2007; 78(8):1568-79. doi: 10.1902/jop.2007.060488 [Crossref] [ Google Scholar]
- Slots J, Ting M. Systemic antibiotics in the treatment of periodontal disease. Periodontol 2000 2002; 28:106-76. doi: 10.1034/j.1600-0757.2002.280106.x [Crossref] [ Google Scholar]
- Kotowska-Rodziewicz A, Zalewska A, Maciejczyk M. A review of preclinical and clinical studies in support of the role of non-steroidal anti-inflammatory drugs in dentistry. Med Sci Monit 2023; 29:e940635. doi: 10.12659/msm.940635 [Crossref] [ Google Scholar]
- Sorsa T, Tervahartiala T, Leppilahti J, Hernandez M, Gamonal J, Tuomainen AM. Collagenase-2 (MMP-8) as a point-of-care biomarker in periodontitis and cardiovascular diseases. Therapeutic response to non-antimicrobial properties of tetracyclines. Pharmacol Res 2011; 63(2):108-13. doi: 10.1016/j.phrs.2010.10.005 [Crossref] [ Google Scholar]
- Noguchi K, Ishikawa I. The roles of cyclooxygenase-2 and prostaglandin E2 in periodontal disease. Periodontol 2000 2007; 43:85-101. doi: 10.1111/j.1600-0757.2006.00170.x [Crossref] [ Google Scholar]
- Preshaw PM, Hefti AF, Jepsen S, Etienne D, Walker C, Bradshaw MH. Subantimicrobial dose doxycycline as adjunctive treatment for periodontitis. A review. J Clin Periodontol 2004; 31(9):697-707. doi: 10.1111/j.1600-051X.2004.00558.x [Crossref] [ Google Scholar]
- Patel VF, Liu F, Brown MB. Advances in oral transmucosal drug delivery. J Control Release 2011; 153(2):106-16. doi: 10.1016/j.jconrel.2011.01.027 [Crossref] [ Google Scholar]
- Joshi D, Garg T, Goyal AK, Rath G. Advanced drug delivery approaches against periodontitis. Drug Deliv 2016; 23(2):363-77. doi: 10.3109/10717544.2014.935531 [Crossref] [ Google Scholar]
- Ashique S, Hussain A, Khan T, Pal S, Rihan M, Farid A. Insights into intra periodontal pocket pathogenesis, treatment, in vitro-in vivo models, products and patents, challenges and opportunity. AAPS PharmSciTech 2024; 25(5):121. doi: 10.1208/s12249-024-02842-6 [Crossref] [ Google Scholar]