J Adv Periodontol Implant Dent. 18(1):55-69.
doi: 10.34172/japid.025.3805
Review Article
Efficacy of different suturing techniques on gingival grafts: A scoping review
Mina Shekarian Data curation, Software, Writing – original draft, Writing – review & editing, 1# 
Shiva Shekarian Data curation, Writing – original draft, Writing – review & editing, 2#
Mahboobe Heydari Software, Validation, 3, 4
Zohreh Afshari Conceptualization, Investigation, Methodology, Supervision, Writing – original draft, Writing – review & editing, 5, *
Romina Meshkinnejad Writing – original draft, Writing – review & editing, 6
Author information:
1Dental Research Center, Dental Research Institute, School of Dentistry, Isfahan University of Medical Sciences, Isfahan, Iran
2School of Dentistry, Shahid Beheshti University of Medical Sciences, Tehran, Iran
3Dental Implants Research Center, Dental Research Institute, School of Dentistry, Isfahan University of Medical Sciences, Isfahan, Iran
4School of Management and Medical Informatics, Isfahan University of Medical Sciences, Isfahan, Iran
5Department of Periodontics, Dental Implants Research Center, Dental Research Institute, School of Dentistry, Isfahan University of Medical Sciences, Isfahan, Iran
6Dental Students’ Research Committee, Department of Periodontics, School of Dentistry, Isfahan University of Medical Sciences, Isfahan, Iran
*
Corresponding author: Zohreh Afshari, Email:
z.afshar90@yahoo.com
# Shared first authorship; both contributed equally to this work.
Abstract
Background.
This review evaluated the efficacy of various suturing techniques in gingival graft stabilization to optimize clinical outcomes and minimize the need for revision surgeries.
Methods.
This scoping review was conducted across Scopus, PubMed, Cochrane, Web of Science, and ProQuest (through April 2025) using PICO criteria: Population (gingival grafts around teeth), Intervention (different suturing techniques), Comparison (efficacy of various suturing techniques in gingival graft stabilization), and Outcomes (keratinized tissue width [KTW], keratinized tissue height [KTH], and root coverage [RC]). From 838 initial records, 73 studies met the inclusion criteria after dual-reviewer screening with arbitration by a third reviewer. Study quality was assessed using the Joanna Briggs Institute tools.
Results.
For free gingival grafts (FGGs), primary stabilization methods included interrupted sutures (with/without periosteal fixation), sling sutures, and cyanoacrylate. Connective tissue grafts (CTGs) predominantly use sling sutures, often combined with cross-mattress or interrupted sutures, vertical/double-cross mattress techniques, or continuous sutures with coronally advanced/tunnel flaps. While 72% of FGG studies (23/32) reported significant KTW improvement with interrupted sutures (a mean gain of 2.1±0.8 mm), CTG studies demonstrated 96% RC success (43/45) with sling-based techniques. However, outcomes showed substantial heterogeneity due to variability in the Miller classification (33/67 studies focused on Class I only) and inconsistent reporting of suture material (only 5/67 specified size/type).
Conclusion.
No single suturing technique demonstrated clear superiority in graft stabilization, likely due to study heterogeneity. While sling/mattress combinations showed optimal RC for CTGs and interrupted sutures/cyanoacrylate performed well for FGGs, standardized RCTs controlling for confounding variables are required to establish definitive protocols.
Keywords: Connective tissue, Gingival grafting, Gingival recession, Sutures, Wound healing
Copyright and License Information
© 2026 The Author(s).
This is an open access article distributed under the terms of the Creative Commons Attribution License (
http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Funding Statement
The present study was funded by Isfahan University of Medical Sciences. It was conducted and supported by a university grant under the code: IR.MUI.DHMT.REC.1403.133.
Introduction
Gingival grafting is a frequently performed procedure in periodontal surgery to repair lost gingival tissue. Gingival grafts are classified into three main categories: autografts, xenografts, and allografts, each with its subgroups. The two most used types of gingival autografts are free gingival grafts (FGGs) and connective tissue grafts (CTGs).1
FGG is ideal for areas with low aesthetic demands or when a significant volume of keratinized tissue is required.2 Additionally, FGG has a low risk of complications and can be easily harvested. However, some drawbacks of FGG include donor site morbidity, limited blood supply, and difficulty in achieving an aesthetically pleasing outcome due to poor color matching.3-6
CTG is suitable for areas with high aesthetic demands or where precise contouring is needed due to its thinner tissue biotype.2 Its applications include increasing the gingival width,7 root coverage (RC),8,9 alveolar ridge augmentation,10,11 addressing peri-implant tissue abnormalities,12 and even coverage of fenestration.13 Additionally, CTG has a better blood supply, leading to faster healing and improved tissue integration compared to FGG.2
Suturing technique plays a critical role in gingival graft success by ensuring tissue stabilization. The main groups of suturing methods include periosteal suture, interrupted suture, sling suture, mattress suture, cross-suture, and continuous suture.
This review examines the efficacy of various types of sutures for gingival graft stabilization, aiming to enhance clinical outcomes and minimize the need for revision surgeries.
Methods
A systematic scoping review of clinical trials was developed, considering the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-analyses) extension for scoping reviews.14 The protocol of this study was based on the framework proposed by Peters et al15 according to the Joanna Briggs Institute. The protocol was registered in Open Science with the code number 10.17605/OSF.IO/4YR9F. In addition, this project was approved by the Ethics Committee of Isfahan University of Medical Sciences (IR.MUI.DHMT.REC.1403.133).
This scoping review aimed to respond to the following focused question. In patients undergoing soft tissue grafts, (a) what methods are used for graft stabilization? (b) What is the efficacy of different suturing techniques on graft success?
The PICO for the present review was as follows:
-
Population (gingival grafts around teeth)
-
Intervention (different suturing techniques)
-
Comparison (efficacy of various suturing techniques in gingival graft stabilization)
-
Outcomes (keratinized tissue width [KTW], keratinized tissue height [KTH], RC).
Selection criteria
We included randomized and non-randomized controlled clinical trials, cohort studies, case reports, and case series that considered at least one type of soft tissue grafting techniques and mentioned the suturing method. Only studies written in English were included. Exclusion criteria included animal studies, in vitro studies, finite element analysis (FEA) studies, letters to the editor, reviews, and publications about soft tissue grafts around dental implants.
Search strategy
An electronic search of articles in English, with no time restrictions, was conducted in Scopus, PubMed, Cochrane, Web of Science, and ProQuest, up to April 2025. The following search model was accomplished using Boolean operators (“Gingival graft*” OR FGG OR “Free gingival graft” OR CTG OR “Connective Tissue graft” OR “Phenotype Modification gingival”) AND Suture* in TITLE/SUBJECT/ABSTRACT based on the particular search strategy of each database (Table 1). A manual search (2000–2025) was performed in the Journal of Dental Research, Journal of Clinical Periodontology, Journal of Periodontology, Clinical Oral Implant Research, Clinical Implant Dentistry and Related Research, International Journal of Oral and Maxillofacial Implants, and Journal of Oral and Maxillofacial Surgery. Additionally, the reference section of the included studies (cross-referencing) was screened for potential further studies.
Screening
After removing duplicates, both automatically (by using Mendeley reference manager software (Version 2.110.2) and manually, the titles and abstracts of the search results were initially screened by two independent authors (M.SH. and SH.SH.). Publications were included for full-text evaluation if the study met the inclusion criteria during the initial analysis or for studies with insufficient information from the title and abstract. Disagreements between the authors were resolved by discussion. In the event of disagreement, the opinion of a third reviewer (Z.A.) was sought. Following full-text assessment, studies were either selected for inclusion or rejected. In papers that included inadequate or limited information about suturing technique, the corresponding authors were contacted via email for clarification or to request missing data, and a reminder was sent twice later.
Data extraction
The following data were extracted from the included studies for further investigations, which are summarized in Table 2: First author, country, study design, number of patients/teeth, site of grafting, grafting technique, type of suture, reported outcomes (KTW, gingival tissue thickness [GTT], clinical attachment level [CAL], KTH, probing depth [PD], attached gingiva [AG], RC, recession depth [RD] and other relative outcomes).
Outcome measures
The primaryoutcomes were GTT and KTW. The secondaryoutcomes included all other reported measures: CAL, PD, RC, KTH, and vestibular depth (VD).
Results
The PRISMA flow diagram illustrates the study selection process at various stages, as depicted in Figure 1.
Some studies meeting our subject criteria were excluded because their suturing techniques were unclear. Although we contacted the corresponding authors for clarification via email, no responses were received, necessitating their exclusion.71,88-90
Figure 2 presents the frequencies of the included articles from 1998 to 2025. Figure 3 presents the frequencies and relationships between the keywords of the articles.
Free gingival graft
Research on the use of the FGG technique for soft tissue augmentation includes three case report studies,39 seventeen randomized controlled trials (RCTs),29,33,42,45,56,57,61-63,67,68,70,82,86,87,91,92one technical note study,48 and two case series.4,9 These studies employed various techniques to stabilize the FGG, such as interrupted sutures (direct loop), sling sutures, modified sling suture, and adhesive materials like cyanoacrylate (Figure 4). Below, the outcomes are organized by clinical parameters, along with the studies that measured them.
Studies that measured PD reported mixed results: while Agrawal et al,67 Goel et al,61 and Barbosa et al29 found no significant change in PD, Menceva et al92 and Chelearescu et al57 observed a reduction in PD. Conversely, Carnio et al45 and Remya et al4 reported a significant increase in PD.
KTW was a commonly measured parameter, with most studies reporting an increase.39,45,57,61,62,67,82,86,87,92 However, some studies found no significant changes in KTW.29,61
CAL was evaluated in several studies, with varying outcomes: Goel et al,61 Kang et al,62 and Remya et al4 reported improvements in CAL, whereas Agrawal et al,67 Yilmaz et al,86 and Barbosa et al29 found no significant changes.
Gingival recession (GR) was another key parameter, with most studies reporting a reduction.57,61,62,67,92 However, some studies found no significant difference between the groups.29,61
RC and complete root coverage (CRC) were evaluated in a subset of studies: Cortellini et al,37 Chelearescu et al,57 and Remya et al4 achieved RC, while Chelearescu et al57 and Shakiliyeva et al87also reported achieving CRC.
GTT was measured in a few studies, with Goel et al61 and César Neto et al82 reporting an increase in GTT.
Some studies focused on postoperative outcomes, such as pain and shrinkage: Alhourani et al68 reported that pain persisted for up to 4 days, with complete healing within 2 months, and noted that the cyanoacrylate group experienced less pain at 6 hours but no significant difference in long-term outcomes. Additionally, the same study observed significantly less shrinkage in the cyanoacrylate group after 3 months.
Table 1.
Specific search strategy for each database
|
Database
|
Search Strategy
|
| Web of Science |
TS = ((“Gingival graft*” OR FGG OR “Free gingival graft” OR CTG OR “Connective Tissue graft” OR “Phenotype Modification gingival”) AND Sutur*) |
| PubMed |
(“Gingival graft*”[Title/Abstract] OR FGG[Title/Abstract] OR “Free gingival graft”[Title/Abstract] OR CTG[Title/Abstract] OR “Connective Tissue graft”[Title/Abstract] OR “Phenotype Modification gingival”[Title/Abstract]) AND Sutur*[Title/Abstract] |
| Scopus |
TITLE-ABS-KEY ((“Gingival graft*” OR FGG OR “Free gingival graft” OR CTG OR “Connective Tissue graft” OR “Phenotype Modification gingival”) AND Sutur*) |
| Embase |
(‘Gingival graft*’:ti,ab,kw OR FGG:ti,ab,kw OR ‘Free gingival graft’:ti,ab,kw OR CTG:ti,ab,kw OR ‘Connective Tissue graft’:ti,ab,kw OR ‘Phenotype Modification gingival’:ti,ab,kw) AND (Sutur*:ti,ab,kw) |
| ProQuest |
((“Gingival graft*” OR FGG OR “Free gingival graft” OR CTG OR “Connective Tissue graft” OR “Phenotype Modification gingival”) AND Sutur*) |
Table 2.
Detailed characteristics of included articles
|
Author (Year)
|
Study design
|
Recession site
|
N. Patients /sites-teeth
|
Graft technique
|
Outcome measures
|
Nelson
(1987)16 |
Case series |
Not mention |
14 P |
CTG + Double pedicle |
CRC, RC |
Grisdale
(1998)17 |
Case report |
Case 1: Mandibular incisors
Case 2: Biopsy site |
2 P |
Case 1: FGG
Case 2: FGG |
RC |
Rosetti et al
(2000)18 |
RCT |
Miller Class I or II gingival recession (upper canine or premolars) |
24 S |
Group 1: CTG + CAF
Group 2: GTR |
KTW, PD, RC,
PI, GI |
Cordioli et al
(2001)19 |
RCT |
Miller Class I or II gingival recession |
21 P /62 S |
Group 1: CTG + Envelope
Group 2: CTG + CAF |
KTW, RC |
Tal et al
(2002)20 |
RCT |
Class I or II Miller classification ≥ 4 mm in the apicocoronal dimension |
14 P |
Group 1: ADM + CAF
Group 2: CTG + CAF |
RD, RW, KTW, PD, CAL |
Carnio et al
(2002)21 |
Case series |
Miller’s Class II and III gingival recession |
4 T |
CTG + EMD + CAF |
PD, CAL, KTW |
| Paolantonio (2002)22 |
RCT |
Miller Class I or II gingival recession |
45 S |
CTG + CAF |
PD, CAL, KTW, GTT |
McGuire & Nunn
(2003)23 |
RCT |
Miller’s Class II gingival recession |
17 P |
Group 1: EMD + CAF
Group 2: CTG + CAF |
RD, RW, KTW, PD, CAL |
Cheung & Griffin
(2004)24 |
RCT |
Miller’s Class I or II gingival recession |
15 P / 54 T |
Group 1: Platelet concentration + CAF
Group 2: SCTG + CAF |
VRD, RW, KTW, PD, CAL |
Carvalho et al
(2006)25 |
Case series |
Class I or II adjacent multiple gingival recession |
10 P / 29 S |
CTG + MCAF |
PD, CAL, KTW, RD |
Dembowska & Drozdzik
(2007)26 |
Case series |
Miller’s Class I or II gingival recession |
18 P
48 S |
Group 1: CTG + TUN
Group 2: CTG + TUN |
PI, RW, KTW, PD, RD |
Felipe et al
(2007)27 |
RCT |
Bilateral Miller Cl I and II gingival recession |
15 P |
Group 1: ADM + CAF
Group 2: ADM + CAF without releasing |
PD, CAL, GR, KTW, GTT |
Remya et al
(2008)4 |
Case series |
Early class III gingival recession |
10 P |
FGG |
PD, CAL, RW, RD |
Han et al
(2008)28 |
RCT |
Miller Class I and II gingival recessions |
20 P |
Group 1: exposed CTG
Group 2: CTG + CAF |
RD, PD, CAL, PI, KTW |
Barbosa et al
(2009)29 |
RCT |
Buccal sites of mandibular incisors and Miller’s class I or II recessions |
24 P |
Group 1: cyanoacrylate
Group 2: FGG |
PD, GR, CAL |
Cortellini et al
(2009)30 |
RCT |
Single Miller Class I and II buccal gingival recessions |
85 P |
Group 1: CTG + CAF
Group 2: CAF |
RD, PD, KTW, CAL |
Bittencourt et al
(2009)31 |
RCT |
bilateral Miller Class I gingival recessions (4 mm) in maxillary canines or premolars |
17 P |
Group 1: CTG + CAF
Group 2: Semilunar Coronally Positioned Flap |
RD, RW, PD, CAL, GTT, KTW |
Byun et al
(2009)32 |
RCT |
Class I or II gingival recessions ‡2 mm on anterior teeth and premolars |
20 P |
Group 1: SCTG + CAF
Group 2: SCTG with Epithelial collar + CAF |
PD, REC, CAL, RW, KTW, PI, GI |
Zucchelli et al
(2010)33 |
RCT |
single Miller’s Class I and II RED |
50 P |
Group 1: dFGG + CAF
Group 2: CTG + CAF |
RD, CAL, KTH, GTT |
Aroca et al
(2010)34 |
RCT |
3 adjacent Class III gingival recessions |
20P / 139 S |
Group 1: CTG + MTUN
Group 2: CTG + EMD + MTUN |
PD, REC, CAL, KTW, RW, GI, PI |
Pini-Prato et al
(2010)35 |
Group 2
clinical trial |
multiple recessions on both sides |
13 P |
Group 1: CTG + CAF
Group 2: CAF |
RD, PD, CAL |
Cardaropoli et al
(2012)36 |
RCT |
single Miller’s Class I or II REC |
18 P |
Group 1: CTG + CAF
Group 2: CM + CAF |
REC, CAL, PD GTT, KTW |
Cortellini et al
(2012)37 |
Case series |
12 single + 16 multiple recessions at lower incisors |
19 p / 28 S |
partially epithelialized FGG |
KTW, RD |
Aroca et al
(2013)38 |
RCT |
Multiple adjacent Miller class I and II gingival recession |
22 P |
Group 1: CM + MTUN
Group 2: CTG + MTUN |
RD, RW, CAL, PPD, KTW, GTT |
Kapadia et al
(2013)39 |
Case report |
Labial aspects of mandibular central incisors |
1 P |
FGG |
Attached gingival gaining |
Moka et al
(2014)40 |
RCT |
Miller’s class I gingival recession defects in maxillary teeth. |
20 P |
Group 1: CAF
Group 2: semilunar coronally repositioned flap |
KTW, RD, PD, CAL |
Zuhr et al
(2021)41 |
RCT |
Miller class I or II recessions for |
24 P / 47 S |
Group 1: CTG + TUN
Group 2: EMD + CAF |
PI, GI, PD, RD, KTW |
| Gümüş & Buduneli (2014)42 |
RCT |
one or two lower anterior teeth, Miller Class III–IV recession |
45 P |
Group 1: FGG
Group 2: FGG
Group 3: FGG |
KTW, shrinkage |
Yaman et al
(2015)43 |
Case series |
One or multiple adjacent Miller Class III gingival recessions |
9 P |
CTG + MTUN |
RC, KTW |
Uraz et al
(2015)44 |
RCT |
Miller Class I and/or Class II GR in mandible or maxilla |
20 P |
Group 1: CAF + expanded mesh CTG
Group 2: CAF + PRF |
RC, RW, CAL, and KTW |
Carnio et al
(2015)45 |
RCT |
Not mention |
Group 1: 42 T
Group 2: 35 T |
Group 1: MARF
Group 2: FGG |
GR, PD, KTW |
| Cieślik-Wegemund et al (2016)46 |
RCT |
Miller Class I and II gingival recession |
28 P |
Group 1: CM + TUN
Group 2: CTG + TUN |
CAL, PD, RD, CRC, KTW |
Santoro et al
(2016)47 |
Case report |
Mandibular canine and a maxillary premolar |
2 P |
CAF + CTG + GTR |
KTH, CAL, PD |
Ku & Leem
(2019)48 |
Case report |
Vestibuloplasty
on anterior mandible |
1 P |
FGG + Ti mesh |
VD, KTW |
Agusto et al
(2019)49 |
Case report |
Class II Miller buccal recession on #24 |
1 P |
CTG + Gingival Pedicle With Split-Thickness Tunnel Technique |
KTW, PD |
Do
(2019)50 |
Case report |
Miller Cl I and II recession defects |
1 P |
CTG + VISTA |
KTW, PD, RC |
Damante et al
(2019)51 |
RCT |
Miller’s class I and II recession defects |
17 P / 40 S |
Group 1: CTG + CAF without root conditioning
Group 2: CTG + CAF with root conditioning |
RD, RC, KTW, GTT, PD, CAL |
Baghele
(2019)52 |
Case series |
Not mention |
6 P |
CTG |
Graft stabilization and
survival |
Rasperini et al
(2019)53 |
Case series |
Not mention |
7 P |
TUN |
RC, GTT, and VD |
Khuntia et al
(2020)54 |
Case series |
Miller’s Class I gingival recession |
3 P |
Case 1: PRF + CAF
Case 2: CTG + CAF
Case 3: CAF |
RC |
Bautista et al
(2022)55 |
Case report |
type I gingival recession on the vestibular surface of tooth 23 |
1 P |
CTG + double papilla flap |
RC |
Shammas at al.
(2020)56 |
RCT |
in two quadrants of the mandible (premolar site) |
10P / 20 S |
Group 1: FGG
Group 2: FGG |
PD, KTW |
Chelarescu et al
(2020)57 |
RCT |
gingival recession areas, class I and II Miller recession, with a recession depth of 2-5mm |
12 P / 44 S |
Group 1: FGG
Group 2: CTG + CAF |
RC, KTW, GR |
Rakasevic et al
(2020)58 |
RCT |
Multiple adjacent Type 1 gingival recessions. |
20 P |
Group 1: CM + MTUN
Group 2: CTG + MTUN |
RC, KTW, GTT, RC |
Salem et al
(2020)59 |
RCT |
Maxillary incisors, canines or premolars |
40 P |
Group 1: CTG + CAF
Group 2: CTG + TUN/pouch |
RC, CRC, GTT, KTW, |
Cardoso et al
(2021)60 |
cohort study |
Miller Class I and II/ Cairo RT I) in maxillary or mandibular canines
and pre-molars |
60 P |
CTG + CAF |
RD, RW, KTW, GTT, RC |
Goel et al
(2021)61 |
RCT |
Miller’s Class I and II gingival recession |
48 S |
Group 1: FGG
Group 2: cyanoacrylate |
RD, CAL, KTW |
Kang et al
(2021)62 |
RCT |
Miller’s Class I and II |
300 S |
Group 1: FGG
Group 2: cyanoacrylate |
CAL, KTW |
AlJasser et al
(2021)63 |
RCT |
lower anterior and premolar regions |
22 P |
Group 1: cyanoacrylate
Group 2: FGG |
KTW, GT, graft shrinkage |
Agrawal et al
(2021)64 |
Case report |
Lingual aspect of mandibular lateral incisor |
1 P |
CTG + TUN |
RC, KTW, shrinkage |
Lee et al
(2021)65 |
Case series |
Miller Class I, II, and III gingival recession |
17 P / 27 T |
CTG + CM + modified TUN |
RC |
Rimbert & Barré
(2021)66 |
Case report |
Deep anterior mandibular recession |
1 P |
CTG + modified TUN |
RC, attached gingiva |
Agrawal et al
(2022)67 |
Case series |
Miller class I or II mandibular premolar region |
17 P / 21 S |
Modified FGG |
RD, CAL, KTW, RC, PD |
Alhourani et al
(2022)68 |
RCT |
gingival recession and
the absence of the keratinized gingiva |
12 P / 24 S |
Group 1: cyanoacrylate
Group 2: FGG |
Graft shrinkage, postoperative pain |
Tambe et al
(2022)69 |
Case report |
Miller Class I maxillary buccal gingival recession |
3 cases |
CTG + MTUN |
RD, CRC, KTW |
Carcuac et al
(2023)70 |
RCT |
mandibular incisors |
30 P |
Group 1: Modified FGG
Group 2: FGG |
RD, KTH, CRC |
Alrmali et al
(2023)71 |
RCT |
Mandibular incisor area |
40 P |
Group 1: Modified gingival graft technique
Group 2: FGG |
KTW, GTT, RD, RW, GT, RC |
Danskin et al
(2023)72 |
Case report |
Gingival recession on the lingual surfaces of teeth #22–27 |
1 P |
CTG + TUN |
RC, GTT, VD |
Vilarrasa & Blasi
(2023)73 |
Case report |
lower incisors |
1 P |
CTG + Double laterally moved CAF |
KTW, RC |
Chang et al
(2023)74 |
Case report |
Not mention |
1 P |
bioceramic-based cement + CM + TUN |
RC, CAL, PD |
Kashani et al
(2023)75 |
Case series |
Cairo RT1 |
13 P |
Molar or canine access CAF + CTG |
CRC |
| Guimarães et al (2023)76 |
Case series |
Multiple Miller’s class I, II and III recession |
10 P/ 85 S |
CTG + TUN |
RD, RW, RC, CRC |
Deepika and Thamaraiselvan
(2023)77 |
Cohort study |
Miller’s class I single or multiple tooth gingival recession |
20 P |
CTG + TUN |
GI, PI, healing index, RC, RD |
| Santamaria et al (2025)78 |
Case report |
RT1 |
1 P |
CTG + CAF |
CRC, PD, BOP, CAL, KTW, GTT, PI, GR |
Yadav et al
(2025)79 |
Case report |
RT 1 |
2 P |
labial gingival graft |
RD, PD, KTW, attached gingiva, Postoperative pain, CRC |
Rao et al
(2024)80 |
RCT |
Miller’s class I and II recession |
20 S |
CTG + CAF |
RH, healing index, root coverage aesthetic score |
Ambili et al
(2024)81 |
Case report |
Cairo’s RT2 |
1 P |
FGG + laterally flipped periosteum |
KTW, CRC |
César Neto et al
(2024)82 |
RCT |
Mandibular anterior teeth |
45 P |
FGG |
STT, STV, CA |
Skierska et al
(2024)83 |
RCT |
Maxillary and mandibular anteriors |
30 P |
CTG + TUN |
RC, KTW, GT, RES, MRC |
Devkar et al
(2024)84 |
RCT |
Mandibular anteriors |
40 S |
CTG |
GT, RC |
Lin
(2025)85 |
Case Series |
Maxillary and mandibular anterior |
3 P |
CTG + Double-VISTA |
RC, CAL gain, KT increase |
Yilmaz et al
(2024)86 |
RCT |
Maxillary anterior |
25 P |
Group1: FGG
Group 2: MCAT |
KTW, GT, RC |
Shakiliyeva et al
(2025)87 |
RCT |
Mandibular anterior region |
25 P |
Group 1: Gingival Unit graft
Group 2: CTG |
RC, KTW |
FGG: free gingival graft; CTG: connective tissue graft; RC: root coverage; GT: gingival thickness; VD: vestibular depth; KTW: keratinized tissue width; CAG: clinical attached gingiva; KTH: keratinized tissue height; KTT: keratinized tissue thickness; PD: probing depth; RW: recession width; CAL: clinical attachment level; CRW: coronal recession width; ARW: apical recession width; PI: plaque index; GI: gingival index; RD: recession depth; STT: soft tissue thickness; GR: gingival recession; GRD: gingival recession depth; GRW: gingival recession width; BRW: buccal recession width; RH: recession height; RES; root coverage esthetic score; MARF: modified apically repositioned flap; GT: gingival thickness, STV: soft tissue volume; CA: creeping attachment.
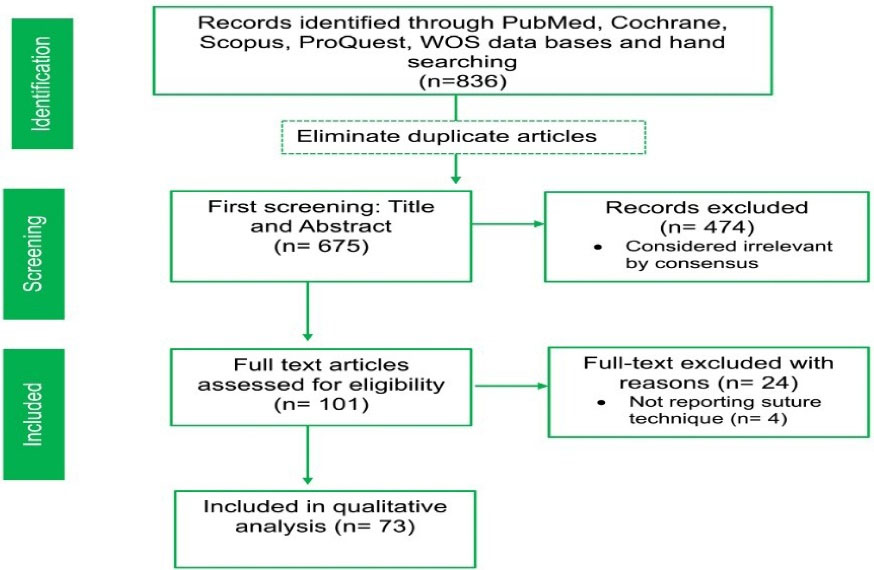
Figure 1.
PRISMA flowchart for selecting articles
.
PRISMA flowchart for selecting articles
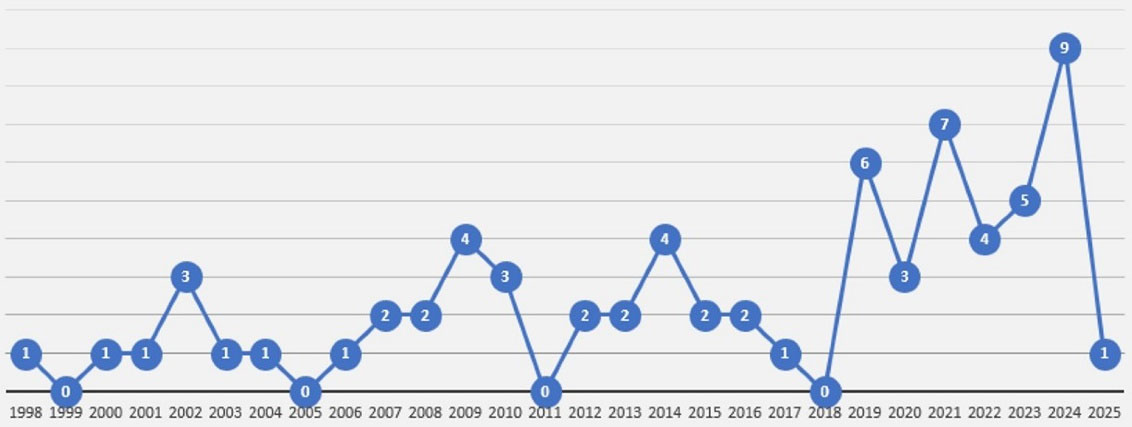
Figure 2.
The frequency of the included articles from 1998 to April 2025
.
The frequency of the included articles from 1998 to April 2025
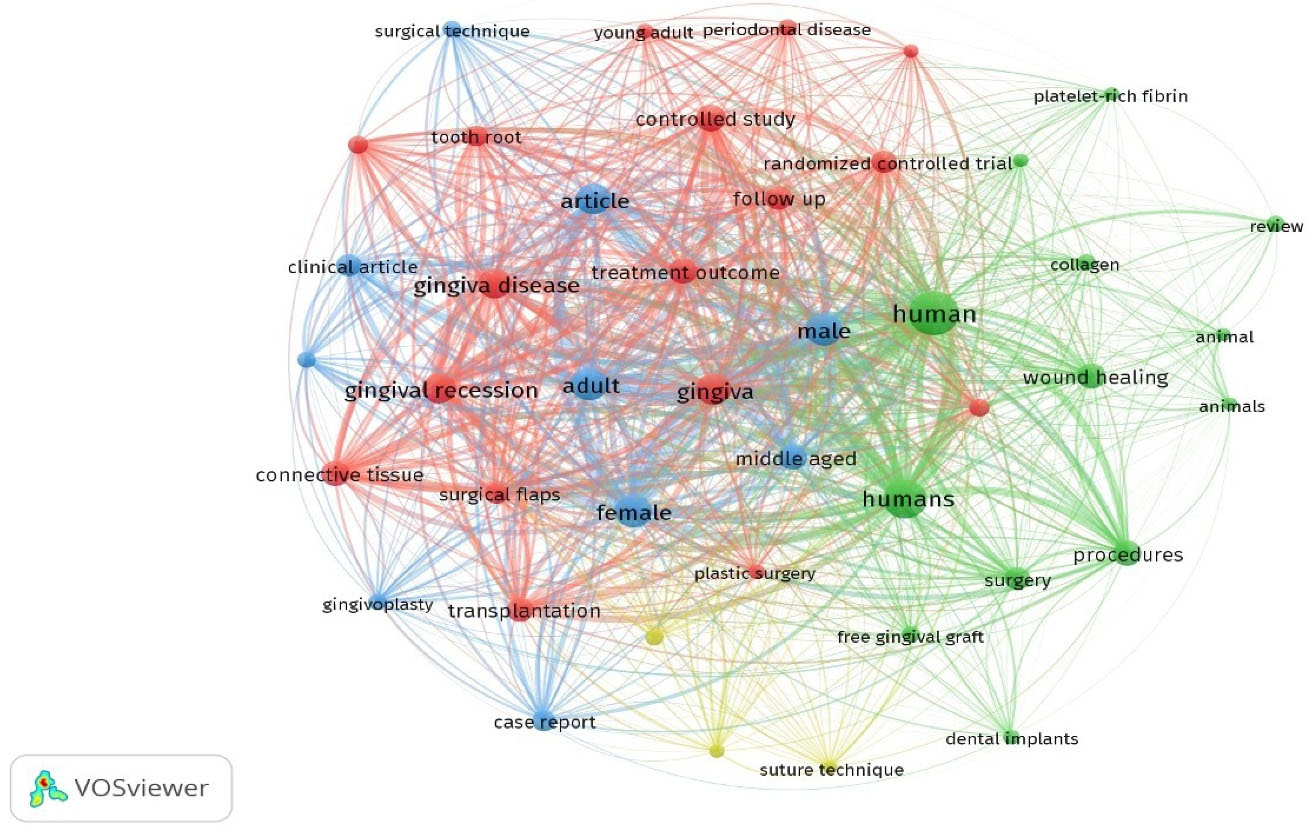
Figure 3.
The frequency and keyword co-occurrence network generated using VOSviewer (version 1.6.20) based on titles and abstracts of the included studies. The data were extracted from the titles and abstracts of all the included articles. The font size and linkage thickness reflect the frequency of each keyword and the strength of co-occurrence between terms, respectively. Larger nodes and bolder text indicate higher frequency and stronger relational clustering within the dataset
.
The frequency and keyword co-occurrence network generated using VOSviewer (version 1.6.20) based on titles and abstracts of the included studies. The data were extracted from the titles and abstracts of all the included articles. The font size and linkage thickness reflect the frequency of each keyword and the strength of co-occurrence between terms, respectively. Larger nodes and bolder text indicate higher frequency and stronger relational clustering within the dataset
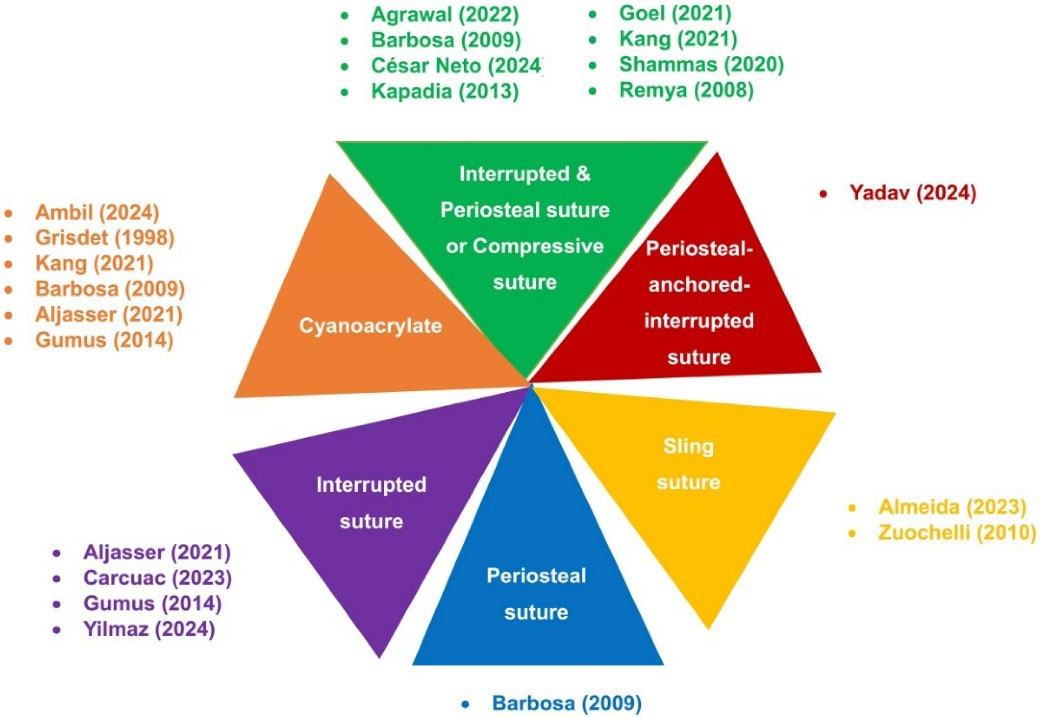
Figure 4.
Various techniques to stabilize the FGG
.
Various techniques to stabilize the FGG
Comparison of sutures vs. cyanoacrylate
Several studies compared sutures with cyanoacrylate for FGG stabilization. While some found no significant differences between the groups,29,61,62 others reported greater RC in the cyanoacrylate group62 and less shrinkage with cyanoacrylate.68
Interrupted sutures for FGG stabilization
Interrupted sutures are the most frequently used technique for stabilizing FGGs. Several studies have investigated the outcomes of this technique, including its impact on VD, keratinized tissue (KT), KTH, RC, and other clinical parameters.
Positive outcomes of interrupted sutures
Interrupted sutures demonstrated several positive outcomes: a technical note study reported an increase in VD and KT,48 while Carcuac et al70 observed an increase in KTH and successful RC.
Comparison of FGG and modified FGG techniques
Carcuac et al70 compared the traditional FGG technique with a modified FGG technique (using a connective tissue pedicle graft under the FGG). The modified FGG group showed a reduction in PD and RD, higher RC and KTH, and significantly lower postoperative morbidity.
César Neto et al82 compared two FGG stabilization approaches: (1) a control group using interrupted sutures with periosteal suspensory sutures over the graft, and (2) a test group where the flap was sutured over the graft without periosteal sutures. Both techniques demonstrated significant increases in soft tissue thickness, with no statistically significant differences between the groups (P > 0.05).
Conflicting findings on interrupted sutures
Despite the positive outcomes reported in many studies, some research has shown conflicting results. AlJasser et al63 found a slight decrease in KTW and a significant reduction in GTT during follow-up assessments. Their comparison of cyanoacrylate and suturing techniques showed no significant differences in mean KTW or mean FGG shrinkage; however, mean GTT increased significantly more in the suturing group.
Comparison of interrupted sutures, cyanoacrylate, and microsurgery
Gümüş and Buduneli42 conducted a study comparing three FGG stabilization techniques: interrupted sutures, cyanoacrylate adhesive, and microsurgery. The interrupted suture group showed a decrease in PD, CAL, plaque index, and papilla bleeding index. In contrast, the cyanoacrylate group exhibited significantly lower graft shrinkage and recipient site pain compared to the other groups. The microsurgery group exhibited graft shrinkage, similar to the interrupted suture group.
Periosteal-anchored Interrupted Suture
Yadav et al79 used a periosteal-anchored interrupted suture technique to stabilize labial gingival grafts for KT augmentation. Their study reported significant gain in keratinized tissue and CRC.
Sling Sutures
Sling sutures are another technique used to secure FGGs.
Outcomes
Keratinized tissue width
Almeida et al91 compared sling sutures (control group) with no sutures (test group). The control group showed a greater increase in KTW, though the difference was not statistically significant.
Yilmaz et al86 demonstrated that FGGs stabilized with sling sutures yield superior long-term KTW gains (3.2 mm) compared to flap techniques.
Modified sling suture
The sling suture with periosteal anchoring87 has demonstrated clinically significant improvements in graft survival, keratinized tissue gains, RC, and healing index compared to conventional sling sutures.87
Cyanoacrylate adhesive
Cyanoacrylate has been explored as an alternative to sutures for FGG stabilization.
Outcomes
Postoperative pain and shrinkage
Alhourani et al68 compared sutures with cyanoacrylate (Iceberg glue). The cyanoacrylate group experienced less postoperative pain at 6 hours and significantly less shrinkage after 3 months, though long-term outcomes were similar.
Compared to sutures, the cyanoacrylate group experienced less postoperative pain at 6 hours and significantly less shrinkage after 3 months, though long-term outcomes were similar.68
No significant differences were found in KTW or graft shrinkage between cyanoacrylate and sutures, but GTT increased significantly more in the suture group.63
When compared to interrupted sutures and microsurgery, cyanoacrylate showed significantly lower graft shrinkage and recipient site pain.42
Cyanoacrylate successfully achieved RC, with one study reporting CRC, increased VD, and reduced tooth morbidity.17,81
CTG
Out of the studies that utilized the CTG technique for gingival reconstruction, twelve case report studies,47,49,50,52,55,64,66,69,72,73,84,85 six case series,21,25,26,43,54 one cohort study,60 twenty-five RCT studies,18-20,22,23,28,30-34,36,38,40,41,44,46,51,57-59,65,74,83 and a non-randomized controlled clinical trial35 were included. CTG secured with numerous suture methods and covered with various techniques, including tunnel flap, coronally advanced flap (CAF) and its modifications, lateral pedicle in addition to tunnel technique, semilunar coronally positioned flap, double papilla, and double pedicle in studies (Supplementary file 1, Table S1).
Tunnel flap technique
While the tunnel and CAF techniques are commonly used in conjunction with CTG, a lack of uniformity is observed in securing the CTG or the entire graft complex in studies. Various suturing methods, such as sling, vertical mattress, double cross, horizontal mattress, V-reverse suture, and interrupted suture, have been utilized to secure the tunnel and its modification flaps.
Sling
Most studies using the tunnel technique flap employed either sling sutures or a combination of sling sutures and another type of suture to secure the graft in place.23,46,53,64,72,83 All research that used only sling sutures found an improvement in RC.46,53,72,76,77,83 Furthermore, an increase in KTW,46,83 and GTT,53as well as a decrease in RD,46 were observed.
Cieślik-Wegemund et al46compared the CTG and CM in their study and demonstrated that RC significantly increased in both groups. However, the mean RD showed a greater increase in the CM group; the mean RC and CRC increased significantly in the CTG group. The mean KTW increased almost equally in both groups.
Sling in addition to cross-mattress
Agrawal et al64 used a sling suture in addition to a cross-mattress to secure the graft from lingual direction and reported that RC, KTW, and GT increased.
Vertical mattress suture
Dembowska and Drozdzik26 reported an increase in KTW and RC similar to the Agrawal study; however, they used different suture methods (vertical mattress).
Double-cross suture
Zuhr et al41 conducted a study comparing the tunnel technique with CTG and CAF with enamel matrix derivative (EMD) for RC. They used a double-crossed suture, along with interrupted sutures, to secure the grafts. The study reported that the tunnel technique with CTG had significantly better results. Both methods showed an increase in RC and a decrease in RD and CAL. However, there was a significant difference in RD and CAL between the tunnel flap with CTG and CAF with EMD. Additionally, the KTW increased in the tunnel flap with CTG but decreased in CAF with EMD.
Interrupted
Salem et al59 conducted a study using interrupted sutures to secure the CTG in both the tunnel technique (TUN) and CAF techniques for treating GR. The study reported that TUN represented better long-term results. While TUN showed GT and KT were significantly better, there was no significant difference in RC between the two groups.
TUN modification techniques
Outcomes by clinical parameter
Several studies have explored the use of TUN modification techniques for harvesting and stabilizing CTGs. Below, the findings are organized by clinical parameters and the studies that measured them.
Studies evaluating RC and CRC demonstrated consistent improvements across various techniques. Using a coronally advanced modified tunnel technique with a horizontal mattress suture, improved RC and CAL were reported.34 Similarly, the MCAT technique combined with site-specific de-epithelialized gingival grafts (DGGs) and sling sutures demonstrated improved RC outcomes.84
When comparing the CTG (control group) and CM (test group), the CTG group showed significantly higher CRC and mean RC.38 A similar comparison found improved RC in both groups, but the CTG group had significantly higher mean RC and CRC.58
The use of bioceramics-based cement with CM also resulted in increased RC.93 Advanced techniques, such as TUN modification with interrupted sutures,65 a modified TUN technique with a V-reverse suture,69 and a double-crossed suture with the MCAT technique43 further enhanced RC and achieved CRC. Additionally, the VISTA approach, which incorporates a subperiosteal sling suture and horizontal mattress suture, resulted in increased RC.50,83
When comparing double-VISTA (featuring dual vestibular incisions and subperiosteal tunneling) with CTG to conventional techniques, the double-VISTA group demonstrated significantly greater mean RC and CRC.85
Studies evaluating KTW reported varied outcomes depending on the technique used. A coronally advanced modified tunnel technique showed no significant changes in KTW,34 while the CM group demonstrated an insignificant increase in KTW.38 Both CTG and CM groups exhibited improved KTW, with no significant differences between them.58 Significant increases in KTW were achieved using advanced techniques, such as a modified TUN technique with a V-reverse suture,69 a double-crossed suture with the MCAT technique,43 a sling suture with MCAT,84 a double-VISTA technique,85 and the VISTA approach, which incorporated advanced suturing methods.50
Studies evaluating CAL demonstrated improvements across various techniques. Using a coronally advanced modified tunnel technique, improved CAL was reported.34 The MCAT technique also showed a significant reduction in CAL.38 When comparing CTG (control group) and CM (test group), both groups exhibited improved CAL, with no significant difference between them.58
Studies evaluating gingival thickness (GT) demonstrated improvements across various techniques. The MCAT technique resulted in a significant increase in GT.38,84 When comparing CTG (control group) and CM (test group), both groups exhibited improved GT, with no significant difference between them.58
Studies evaluating PD showed consistent stability across different techniques. Using a coronally advanced modified tunnel technique, no significant change in PD was reported.34 Similarly, the MCAT technique also resulted in PD remaining almost unchanged.38
Studies evaluating gingival recession depth (GRD) and gingival recession width (GRW) demonstrated significant improvements across various techniques. The MCAT technique resulted in a significant reduction in both GRD and GRW.28 When comparing CTG (control group) and CM (test group), both groups exhibited improved GRD and GRW, with no significant difference between them.58
Studies evaluating the plaque index (PI) and the gingival index (GI) have shown consistent stability. Using a coronally advanced modified tunnel technique, no significant changes in PI or GI were reported.34
Postoperative outcomes
Postoperative outcomes were evaluated in several studies, with positive results reported across different techniques. Tambe et al69 achieved CRC and increased KTW with minimal postoperative complications using a modified TUN technique with a V-reverse suture. Also, Skierska et al83 demonstrated that adding cross-linked hyaluronic acid (HA) to the tunnel technique with CTG significantly improved outcomes compared to CTG alone. The HA-enhanced group demonstrated superior RC, a greater gain in KTW, and faster healing with reduced inflammation.
According to Lin,85 the double-VISTA approach further optimized patient experiences, with higher satisfaction and lower postoperative pain. Similarly, Devkar et al84 demonstrated that the MCAT technique with DGG yielded predictable outcomes, including uneventful healing and enhanced aesthetic results. These findings align with outcomes from the standard VISTA technique,94 which incorporated a subperiosteal sling suture and horizontal mattress suture and improved the stability of the CTG and flap complex, leading to better RC and KTW.50
Coronally advanced flap for CTG stabilization
Outcomes by clinical parameter
The CAF technique, often combined with CTGs, has been widely studied for treating GR. Below, the findings are organized by clinical parameters and the studies that measured them.
RC and CRC were evaluated across multiple studies using various suturing techniques. Studies using sling sutures reported improved RC,20,25,32,33,44with some also achieving improved CRC.30,35 Combining sling and interrupted sutures further enhanced RC,21,23,73 particularly in the CTG group, which showed higher CRC compared to other groups.30,35
Studies using interrupted sutures alone have also demonstrated improved RC,19,59 while advanced techniques, such as continuous and vertical mattress sutures, have contributed to similaroutcomes.57 Additionally, the use of continuous vertical mattress and sling sutures resulted in improved RC,24 highlighting the effectiveness of advanced suturing methods.
KTW outcomes varied across studies, depending on the suturing technique used. Studies employing sling sutures reported mixed results: Byun et al32 and Tal et al20 observed an increase in KTW, while Cardoso et al60 noted a decrease. For studies combining sling and interrupted sutures, Vilarrasa & Blasi73 and McGuire & Nunn23 reported an increase in KTW. Similarly, studies using interrupted sutures, such as those by Cordioli et al19 and Salem et al,59 also demonstrated an increase in KTW. Additionally, Chelearescu et al57 achieved an increased KTW with continuous and vertical mattress sutures, and Cheung & Griffin.24 reported improved KTW using continuous vertical mattress and sling sutures.
RD and recession width (RW) significantly decreased across studies using various suturing techniques. Studies employing sling sutures reported reductions in RD and RW.32,33,44,60 Similarly, studies combining sling and interrupted sutures also observed reductions in RD.21,73 Additionally, the use of continuous vertical mattress and sling sutures resulted in reductions in RD.24
CAL improved across studies using various suturing techniques. Studies employing sling sutures reported improvements in CAL.25,32,33,44 Similarly, studies combining sling and interrupted sutures also revealed improvements in CAL.21 Additionally, the use of continuous vertical mattress and sling sutures resulted in improvements in CAL.24
GT and GTT were evaluated across studies using different suturing techniques. Studies employing sling sutures, such as that by Cardoso et al,60 reported an increase in GT. In contrast, those combining sling and interrupted sutures, including a study by Vilarrasa and Blasi,73 observed an increase in GTT. Similarly, studies using interrupted sutures, such as that by Salem et al,59 also demonstrated an increase in GTT.
Regarding PD, studies using sling sutures, including those by Byun et al,32 Tal et al,20 and Zucchelli et al,33 reported no significant changes in PD. Similarly, studies combining sling and interrupted sutures, such as that by Carnio et al,21 also found no significant changes in PD. However, Cheung and Griffin24 observed a decrease in PD using continuous vertical mattress and sling sutures.
PI and GI were evaluated in studies using sling sutures, with Byun et al32 reporting no significant changes in either PI or GI.
Other techniques
Outcomes by surgical technique
Several studies have explored advanced flap techniques and alternative methods for RC, often combined with CTGs or other materials (Tables S2 and S3). Below, the findings are organized by surgical techniques and their associated outcomes.
The TUN technique resulted in improved RC, increased GTT, and VD.53
A novel technique combining the lateral pedicle with a tunnel flap achieved CRC and excellent esthetic outcomes for single deep recessions on mandibular incisors.49
Comparing a semilunar coronally positioned flap with adhesive to CTG with micro-sutures, the CTG group showed significantly increased GTT, with no significant differences in RC between the groups. Both groups demonstrated improvements in RD, RW, KTW, PD, and CAL, though differences were not statistically significant.31
The double papilla technique, using a sling and interrupted sutures, resulted in 100% RC.55
Using the double pedicle technique with sling, cross sling, and interrupted sutures, significant improvements were observed in GR, CAL, KTW, and GTT, with 90% RC and 60% CRC.22 Another study using a similar technique achieved CRC rates of 50% (advanced recession), 67% (moderate recession), and 100% (slight recession).16
PRF with CAF was used to treat Miller’s class I recessions, resulting in a significant increase in AG and 5 mm of CAL.54
Comparing CAF with two releasing incisions to a modified technique using horizontal incisions, the CAF group showed significantly better RC (84.81% vs. 68.98% in the test group). Both groups demonstrated a significant reduction in GR, gain in CAL, and an increase in KTT, with no significant changes in other clinical parameters.27
A new approach combining a modified tunnel technique with simultaneous frenuloplasty stabilized the CTG with internal mattress sutures and advanced the flap coronally using vertical double-crossed sutures, achieving CRC.66
The lingually-tied horizontal mattress contouring suture, a new suturing technique, stabilized the CTG with a sling-like configuration, resulting in long-term graft survival and stabilization.52
Two cases of combined regenerative and mucogingival treatment for deep intrabony defects used deproteinized bovine bone xenograft and CTG secured with horizontal mattress sutures, achieving remarkable RC, KTH, GTT, and CAL two years postoperatively.47
Comparing CAF (using sling and interrupted sutures) to SCRF (left unbound without sutures), the CAF group showed better outcomes in CAL, RC, CRC, and esthetics, while the SCRF group demonstrated a significant increase in KTW.40
Discussion
The current scoping review aimed to investigate the impact of various suturing techniques on tissue stabilization and clinical healing outcomes following surgery. A total of 63 studies meeting the inclusion criteria were analyzed, with a focus on measuring KTW and GTT.
Various suturing methods, including periosteal suture, interrupted suture, sling suture, mattress suture, cross-suture, and continuous suture, were examined to determine whether the technique used significantly influenced tissue stabilization.
The information gathered in this study ranges from a collection of case report studies to RCTs where various parameters such as KTW, CAL, and PD have been investigated, with detailed information provided in the results section. Additionally, some studies have examined other parameters, such as tissue shrinkage and patient pain postoperatively. These parameters should be considered in future studies for further investigations.
Key limitations included variability in suture materials, the Miller classification of GR, and surgical site selection in the dental area during surgery, as well as the duration of surgery across different studies, which could potentially reduce the study’s accuracy.
Based on the provided search results, it appears that while some studies, such as that by Agusto et al,49 have mentioned the suture material, most studies do not specify the suture material or needle size used. According to Baghele52 the choice of suture depends on factors such as the biological interactions of the materials, tissue configuration, and the biomechanical properties of the wound. Carvalho et al25 used 5-0 polyglactin 910 Vicryl sutures for CTG stabilization using a sling suture technique. Baghele52 believe that, in various suturing techniques, 4-0, 5-0, or 6-0 absorbable sutures can be used. Furthermore, if the surgeon does not use magnifying instruments, 4-0 and 5-0 sutures are more comfortable to work with.
One of the other challenges involves GR according to the Miller classification.
Thirty-three articles focused on Miller class I GRs,18-20,22-33,36,38,40,41,44,46,50,51,54,55,57,58,60-62,65,67,69 twenty-nine worked on Miller class II GRs,18-30,32,33,36,38,41,44,46,49,50,51,57,60-62,65,67 and six determined class III GRs;4,21,34,43,65,76,81 Miller class IV recession was addressed in just one article.76 As we know, a higher Miller classification indicates more GR in that area, leading to lower expectations of CRC after surgery. Additionally, the surgical site is crucial because, for instance, performing surgery in the mandibular incisor region, due to poor mucogingival conditions of the lower jaw,67 especially on the lingual side, is significantly more challenging than surgery in other areas.
Lastly, the duration of surgery is another influential factor. For instance, procedures using cyanoacrylate required less operating time due to its ease of application compared to traditional suturing techniques.62,63 Conversely, longer procedures were associated with sutures that required additional steps, such as sealing contact points with composite resin.38
One of the discrepancies in this study was the lack of RCTs for some techniques, with only case reports available for certain methods. The gold standard for evaluating the effect of suturing techniques on tissue stability is RCTs in which all parameters are kept constant, and only the suturing techniques vary. This type of study design allows for a direct comparison of the efficacy of different suturing techniques while minimizing the influence of confounding factors. Based on our research, only one study has investigated the impact of various suturing techniques on grafts. However, this study only looked at the effect of suture type on the shrinkage of FGG and did not consider other factors.56
Several factors, including the surgeon’s expertise and individual practices, significantly influence surgical outcomes in this context. Almeida et al91 mentioned that less experienced surgeons prefer to use “X” sutures anchored in the periosteum, while the modified technique eliminates the need for periosteal sutures.
Conclusion
The suturing technique did not appear to be a definitive factor in graft stabilization, which can be due to the existence of highly significant heterogeneity in the studies and other limitations mentioned. Hence, it is advisable to conduct additional controlled RCTs in this field to examine the impact of suture type on graft outcomes.
Competing Interests
The authors deny any conflicts of interest.
Data Availability
The data in this article are available upon request. You can contact the corresponding author to obtain the necessary data (z.afshar90@yahoo.com).
Ethical Approval
The protocol was registered in Open Science with the code 10.17605/OSF.IO/4YR9F. In addition, this study was approved by the Ethics Committee of Isfahan University of Medical Sciences with ethics code IR.MUI.DHMT.REC.1403.133.
Supplementary Files
Supplementary file 1 contains Table S1-S3.
(pdf)
Acknowledgements
The authors gratefully acknowledge the support of Isfahan University of Medical Sciences for this project. We also used Grammarly and ChatGPT (OpenAI) to assist with grammatical corrections and language refinement of the manuscript. During the preparation of this work, the authors used Monica and ChatGPT 4 to correct the structure and grammar. After using these tools, authors reviewed and edited the content as needed and take full responsibility for the content of the publication.
References
- Thoma DS, Benić GI, Zwahlen M, Hämmerle CH, Jung RE. A systematic review assessing soft tissue augmentation techniques. Clin Oral Implants Res 2009; 20 Suppl 4:146-65. doi: 10.1111/j.1600-0501.2009.01784.x [Crossref] [ Google Scholar]
- Puri K, Kumar A, Khatri M, Bansal M, Rehan M, Siddeshappa ST. 44-year journey of palatal connective tissue graft harvest: a narrative review. J Indian Soc Periodontol 2019; 23(5):395-408. doi: 10.4103/jisp.jisp_288_18 [Crossref] [ Google Scholar]
- Miller PD Jr. Root coverage with the free gingival graft. Factors associated with incomplete coverage. J Periodontol 1987; 58(10):674-81. doi: 10.1902/jop.1987.58.10.674 [Crossref] [ Google Scholar]
- Remya V, Kishore Kumar K, Sudharsan S, Arun KV. Free gingival graft in the treatment of class III gingival recession. Indian J Dent Res 2008; 19(3):247-52. doi: 10.4103/0970-9290.42959 [Crossref] [ Google Scholar]
- Silva CO, Ribeiro Edel P, Sallum AW, Tatakis DN. Free gingival grafts: graft shrinkage and donor-site healing in smokers and non-smokers. J Periodontol 2010; 81(5):692-701. doi: 10.1902/jop.2010.090381 [Crossref] [ Google Scholar]
- Wang HL, Bunyaratavej P, Labadie M, Shyr Y, MacNeil RL. Comparison of 2 clinical techniques for treatment of gingival recession. J Periodontol 2001; 72(10):1301-11. doi: 10.1902/jop.2001.72.10.1301 [Crossref] [ Google Scholar]
- Edel A. Clinical evaluation of free connective tissue grafts used to increase the width of keratinised gingiva. J Clin Periodontol 1974; 1(4):185-96. doi: 10.1111/j.1600-051x.1974.tb01257.x [Crossref] [ Google Scholar]
- Harris RJ. The connective tissue and partial thickness double pedicle graft: a predictable method of obtaining root coverage. J Periodontol 1992; 63(5):477-86. doi: 10.1902/jop.1992.63.5.477 [Crossref] [ Google Scholar]
- Langer B, Langer L. Subepithelial connective tissue graft technique for root coverage. J Periodontol 1985; 56(12):715-20. doi: 10.1902/jop.1985.56.12.715 [Crossref] [ Google Scholar]
- Cohen ES. Ridge augmentation utilizing the subepithelial connective tissue graft: case reports. Pract Periodontics Aesthet Dent 1994; 6(2):47-53. [ Google Scholar]
- Orth CF. A modification of the connective tissue graft procedure for the treatment of type II and type III ridge deformities. Int J Periodontics Restorative Dent 1996; 16(3):266-77. [ Google Scholar]
- Edel A. The use of a connective tissue graft for closure over an immediate implant covered with occlusive membrane. Clin Oral Implants Res 1995; 6(1):60-5. doi: 10.1034/j.1600-0501.1995.060108.x [Crossref] [ Google Scholar]
- Tewari S, Dhiman M, Bhagavatheeswaran S, Thakur V, Tewari S. Management of isolated labial mucosal fenestration by endodontic microsurgery along with platelet-rich fibrin and connective tissue graft: a series of four cases. Clin Adv Periodontics 2022; 12(3):194-203. doi: 10.1002/cap.10194 [Crossref] [ Google Scholar]
- Tricco AC, Lillie E, Zarin W, O’Brien KK, Colquhoun H, Levac D. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med 2018; 169(7):467-73. doi: 10.7326/m18-0850 [Crossref] [ Google Scholar]
- Peters MD, Godfrey CM, Khalil H, McInerney P, Parker D, Soares CB. Guidance for conducting systematic scoping reviews. Int J Evid Based Healthc 2015; 13(3):141-6. doi: 10.1097/xeb.0000000000000050 [Crossref] [ Google Scholar]
- Nelson SW. The subpedicle connective tissue graft. A bilaminar reconstructive procedure for the coverage of denuded root surfaces. J Periodontol 1987; 58(2):95-102. doi: 10.1902/jop.1987.58.2.95 [Crossref] [ Google Scholar]
- Grisdale J. The use of cyanoacrylates in periodontal therapy. J Can Dent Assoc 1998; 64(9):632-3. [ Google Scholar]
- Rosetti EP, Marcantonio RA, Rossa C Jr, Chaves ES, Goissis G, Marcantonio E Jr. Treatment of gingival recession: comparative study between subepithelial connective tissue graft and guided tissue regeneration. J Periodontol 2000; 71(9):1441-7. doi: 10.1902/jop.2000.71.9.1441 [Crossref] [ Google Scholar]
- Cordioli G, Mortarino C, Chierico A, Grusovin MG, Majzoub Z. Comparison of 2 techniques of subepithelial connective tissue graft in the treatment of gingival recessions. J Periodontol 2001; 72(11):1470-6. doi: 10.1902/jop.2001.72.11.1470 [Crossref] [ Google Scholar]
- Tal H, Moses O, Zohar R, Meir H, Nemcovsky C. Root coverage of advanced gingival recession: a comparative study between acellular dermal matrix allograft and subepithelial connective tissue grafts. J Periodontol 2002; 73(12):1405-11. doi: 10.1902/jop.2002.73.12.1405 [Crossref] [ Google Scholar]
- Carnio J, Camargo PM, Kenney EB, Schenk RK. Histological evaluation of 4 cases of root coverage following a connective tissue graft combined with an enamel matrix derivative preparation. J Periodontol 2002; 73(12):1534-43. doi: 10.1902/jop.2002.73.12.1534 [Crossref] [ Google Scholar]
- Paolantonio M. Treatment of gingival recessions by combined periodontal regenerative technique, guided tissue regeneration, and subpedicle connective tissue graft. A comparative clinical study. J Periodontol 2002; 73(1):53-62. doi: 10.1902/jop.2002.73.1.53 [Crossref] [ Google Scholar]
- McGuire MK, Nunn M. Evaluation of human recession defects treated with coronally advanced flaps and either enamel matrix derivative or connective tissue. Part 1: comparison of clinical parameters. J Periodontol 2003; 74(8):1110-25. doi: 10.1902/jop.2003.74.8.1110 [Crossref] [ Google Scholar]
- Cheung WS, Griffin TJ. A comparative study of root coverage with connective tissue and platelet concentrate grafts: 8-month results. J Periodontol 2004; 75(12):1678-87. doi: 10.1902/jop.2004.75.12.1678 [Crossref] [ Google Scholar]
- Carvalho PF, da Silva RC, Cury PR, Joly JC. Modified coronally advanced flap associated with a subepithelial connective tissue graft for the treatment of adjacent multiple gingival recessions. J Periodontol 2006; 77(11):1901-6. doi: 10.1902/jop.2006.050450 [Crossref] [ Google Scholar]
- Dembowska E, Drozdzik A. Subepithelial connective tissue graft in the treatment of multiple gingival recession. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2007; 104(3):e1-7. doi: 10.1016/j.tripleo.2007.03.013 [Crossref] [ Google Scholar]
- Felipe ME, Andrade PF, Grisi MF, Souza SL, Taba M, Palioto DB. Comparison of two surgical procedures for use of the acellular dermal matrix graft in the treatment of gingival recessions: a randomized controlled clinical study. J Periodontol 2007; 78(7):1209-17. doi: 10.1902/jop.2007.060356 [Crossref] [ Google Scholar]
- Han JS, John V, Blanchard SB, Kowolik MJ, Eckert GJ. Changes in gingival dimensions following connective tissue grafts for root coverage: comparison of two procedures. J Periodontol 2008; 79(8):1346-54. doi: 10.1902/jop.2008.070472 [Crossref] [ Google Scholar]
- Barbosa FI, Corrêa DS, Zenóbio EG, Costa FO, Shibli JA. Dimensional changes between free gingival grafts fixed with ethyl cyanoacrylate and silk sutures. J Int Acad Periodontol 2009; 11(2):170-6. [ Google Scholar]
- Cortellini P, Tonetti M, Baldi C, Francetti L, Rasperini G, Rotundo R. Does placement of a connective tissue graft improve the outcomes of coronally advanced flap for coverage of single gingival recessions in upper anterior teeth? A multi-centre, randomized, double-blind, clinical trial. J Clin Periodontol 2009; 36(1):68-79. doi: 10.1111/j.1600-051X.2008.01346.x [Crossref] [ Google Scholar]
- Bittencourt S, Del Peloso Ribeiro E, Sallum EA, Sallum AW, Nociti FH, Casati MZ. Semilunar coronally positioned flap or subepithelial connective tissue graft for the treatment of gingival recession: a 30-month follow-up study. J Periodontol 2009; 80(7):1076-82. doi: 10.1902/jop.2009.080498 [Crossref] [ Google Scholar]
- Byun HY, Oh TJ, Abuhussein HM, Yamashita J, Soehren SE, Wang HL. Significance of the epithelial collar on the subepithelial connective tissue graft. J Periodontol 2009; 80(6):924-32. doi: 10.1902/jop.2009.080673 [Crossref] [ Google Scholar]
- Zucchelli G, Mele M, Stefanini M, Mazzotti C, Marzadori M, Montebugnoli L. Patient morbidity and root coverage outcome after subepithelial connective tissue and de-epithelialized grafts: a comparative randomized-controlled clinical trial. J Clin Periodontol 2010; 37(8):728-38. doi: 10.1111/j.1600-051X.2010.01550.x [Crossref] [ Google Scholar]
- Aroca S, Keglevich T, Nikolidakis D, Gera I, Nagy K, Azzi R. Treatment of class III multiple gingival recessions: a randomized-clinical trial. J Clin Periodontol 2010; 37(1):88-97. doi: 10.1111/j.1600-051X.2009.01492.x [Crossref] [ Google Scholar]
- Pini-Prato GP, Cairo F, Nieri M, Franceschi D, Rotundo R, Cortellini P. Coronally advanced flap versus connective tissue graft in the treatment of multiple gingival recessions: a split-mouth study with a 5-year follow-up. J Clin Periodontol 2010; 37(7):644-50. doi: 10.1111/j.1600-051X.2010.01559.x [Crossref] [ Google Scholar]
- Cardaropoli D, Tamagnone L, Roffredo A, Gaveglio L. Treatment of gingival recession defects using coronally advanced flap with a porcine collagen matrix compared to coronally advanced flap with connective tissue graft: a randomized controlled clinical trial. J Periodontol 2012; 83(3):321-8. doi: 10.1902/jop.2011.110215 [Crossref] [ Google Scholar]
- Cortellini P, Tonetti M, Prato GP. The partly epithelialized free gingival graft (PE-FGG) at lower incisors. A pilot study with implications for alignment of the mucogingival junction. J Clin Periodontol 2012; 39(7):674-80. doi: 10.1111/j.1600-051X.2012.01896.x [Crossref] [ Google Scholar]
- Aroca S, Molnár B, Windisch P, Gera I, Salvi GE, Nikolidakis D. Treatment of multiple adjacent Miller class I and II gingival recessions with a modified coronally advanced tunnel (MCAT) technique and a collagen matrix or palatal connective tissue graft: a randomized, controlled clinical trial. J Clin Periodontol 2013; 40(7):713-20. doi: 10.1111/jcpe.12112 [Crossref] [ Google Scholar]
- Kapadia JA, Bhedasgoankar SY, Bhandari SD. Periodontal microsurgery: a case report. J Indian Soc Periodontol 2013; 17(6):790-2. doi: 10.4103/0972-124x.124511 [Crossref] [ Google Scholar]
- Moka LR, Boyapati R, M S, D NS, Swarna C, Putcha M. Comparison of coronally advanced and semilunar coronally repositioned flap for the treatment of gingival recession. J Clin Diagn Res 2014; 8(6):ZC04-8. doi: 10.7860/jcdr/2014/8928.4428 [Crossref] [ Google Scholar]
- Zuhr O, Akakpo D, Eickholz P, Vach K, Hürzeler MB, Petsos H. Tunnel technique with connective tissue graft versus coronally advanced flap with enamel matrix derivate for root coverage: 5-year results of an RCT using 3D digital measurement technology for volumetric comparison of soft tissue changes. J Clin Periodontol 2021; 48(7):949-61. doi: 10.1111/jcpe.13470 [Crossref] [ Google Scholar]
- Gümüş P, Buduneli E. Graft stabilization with cyanoacrylate decreases shrinkage of free gingival grafts. Aust Dent J 2014; 59(1):57-64. doi: 10.1111/adj.12149 [Crossref] [ Google Scholar]
- Yaman D, Demirel K, Aksu S, Basegmez C. Treatment of multiple adjacent Miller class III gingival recessions with a modified tunnel technique: a case series. Int J Periodontics Restorative Dent 2015; 35(4):489-97. doi: 10.11607/prd.2049 [Crossref] [ Google Scholar]
- Uraz A, Sezgin Y, Yalim M, Taner IL, Cetiner D. Comparative evaluation of platelet-rich fibrin membrane and connective tissue graft in the treatment of multiple adjacent recession defects: a clinical study. J Dent Sci 2015; 10(1):36-45. doi: 10.1016/j.jds.2012.10.010 [Crossref] [ Google Scholar]
- Carnio J, Camargo PM, Pirih PQ. Surgical techniques to increase the apicocoronal dimension of the attached gingiva: a 1-year comparison between the free gingival graft and the modified apically repositioned flap. Int J Periodontics Restorative Dent 2015; 35(4):571-8. doi: 10.11607/prd.2386 [Crossref] [ Google Scholar]
- Cieślik-Wegemund M, Wierucka-Młynarczyk B, Tanasiewicz M, Gilowski Ł. Tunnel technique with collagen matrix compared with connective tissue graft for treatment of periodontal recession: a randomized clinical trial. J Periodontol 2016; 87(12):1436-43. doi: 10.1902/jop.2016.150676 [Crossref] [ Google Scholar]
- Santoro G, Zucchelli G, Gherlone E. Combined regenerative and mucogingival treatment of deep intrabony defects associated with buccal gingival recession: two case reports. Int J Periodontics Restorative Dent 2016; 36(6):849-57. doi: 10.11607/prd.2764 [Crossref] [ Google Scholar]
- Ku JK, Leem DH. Vestibuloplasty covering titanium mesh with grafted free gingiva on anterior mandible: technical report and rationale. J Korean Assoc Oral Maxillofac Surg 2019; 45(6):369-73. doi: 10.5125/jkaoms.2019.45.6.369 [Crossref] [ Google Scholar]
- Agusto M, Simpson KT, Salman A, Schincaglia GP. Novel surgical approach for root coverage of single deep recessions on mandibular incisors: gingival pedicle with split-thickness tunnel technique. Clin Adv Periodontics 2019; 9(4):166-71. doi: 10.1002/cap.10063 [Crossref] [ Google Scholar]
- Do JH. Connective tissue graft stabilization by subperiosteal sling suture for periodontal plastic surgery using the VISTA approach. Int J Periodontics Restorative Dent 2019; 39(2):253-158. doi: 10.11607/prd.3529 [Crossref] [ Google Scholar]
- Damante CA, Karam P, Ferreira R, Rezende ML, Greghi SL, Sant’Ana AC. Root surface demineralization by citric acid/tetracycline gel and aPDT associated to subepithelial connective tissue graft improves root coverage outcomes. A 12-month preliminary randomized clinical trial.. J Photochem Photobiol B 2019; 197:111528. doi: 10.1016/j.jphotobiol.2019.111528 [Crossref] [ Google Scholar]
- Baghele ON. A detailed description and 16-year validation of a new suturing method for stabilizing connective tissue grafts at recipient sites for root coverage and gingival augmentation. Indian J Dent Res 2019; 30(2):243-8. doi: 10.4103/ijdr.IJDR_614_17 [Crossref] [ Google Scholar]
- Rasperini G, Codari M, Limiroli E, Acunzo R, Tavelli L, Levickiene AZ. Graftless tunnel technique for the treatment of multiple gingival recessions in sites with thick or very thick biotype: a prospective case series. Int J Periodontics Restorative Dent 2019; 39(6):e203-10. doi: 10.11607/prd.4134 [Crossref] [ Google Scholar]
- Khuntia P, Nayak R, Das AC, Mohanty R, Panda S, Das S. Root coverage procedures: a case series. Indian J Forensic Med Toxicol 2020; 14(4):8648-54. doi: 10.37506/ijfmt.v14i4.13063 [Crossref] [ Google Scholar]
- Bautista CA, Cafferata EA, Vernal R, Cárdenas AM. Treatment of a single gingival recession with a subepithelial connective tissue graft with a double papilla flap: a case report. SAGE Open Med Case Rep 2022; 10:2050313x221078706. doi: 10.1177/2050313x221078706 [Crossref] [ Google Scholar]
- Shammas A, Ranjbar H, Solghar MA, Asghari N, Mohammadi M. Horizontal continuous and apical stretching sutures does not reduce FGG shrinkage: a split-mouth randomized controlled clinical trial. Eur Oral Res 2020; 54(1):42-7. doi: 10.26650/eor.20200080 [Crossref] [ Google Scholar]
- Chelarescu S, Vaida C, Ormenisan A, Teodorescu E, Olteanu C, Kantor J. Gingival recession treatment: surgery and chemical compounds. Rev Chim 2020; 71(6):508-18. doi: 10.37358/rc.20.6.8217 [Crossref] [ Google Scholar]
- Rakasevic DL, Milinkovic IZ, Jankovic SM, Soldatovic IA, Aleksic ZM, Nikolic-Jakoba NS. The use of collagen porcine dermal matrix and connective tissue graft with modified coronally advanced tunnel technique in the treatment of multiple adjacent type I gingival recessions: a randomized, controlled clinical trial. J Esthet Restor Dent 2020; 32(7):681-90. doi: 10.1111/jerd.12624 [Crossref] [ Google Scholar]
- Salem S, Salhi L, Seidel L, Lecloux G, Rompen E, Lambert F. Tunnel/pouch versus coronally advanced flap combined with a connective tissue graft for the treatment of maxillary gingival recessions: four-year follow-up of a randomized controlled trial. J Clin Med 2020; 9(8):2641. doi: 10.3390/jcm9082641 [Crossref] [ Google Scholar]
- Cardoso MV, Lara VS, Sant’Ana AC, Damante CA, Ragghianti Zangrando MS. Late complications after root coverage with two types of subepithelial connective tissue grafts, clinical and histopathological evaluation: a prospective cohort study. J Clin Periodontol 2021; 48(3):431-40. doi: 10.1111/jcpe.13413 [Crossref] [ Google Scholar]
- Goel A, Ghai D, Sood A, Singh GP, Nagi PK, Singh P. A comparative evaluation of silk suture and cyanoacrylate adhesive in the stabilization of free gingival graft harvested with erbium: yttrium-aluminum-garnet laser: a clinical study. J Pharm Bioallied Sci 2021; 13(Suppl 2):S1672-8. doi: 10.4103/jpbs.jpbs_404_21 [Crossref] [ Google Scholar]
- Kang J, Yi M, Chen J, Peng M. Comparative assessment between bio-adhesive material and silk suture in regard to healing, clinical attachment level and width of keratinized gingiva in gingival recession defects cases. Sci Prog 2021; 104(2):368504211011868. doi: 10.1177/00368504211011868 [Crossref] [ Google Scholar]
- AlJasser RN, AlSarhan MA, AlOtaibi DH, AlOraini S, AlNuwaiser R, AlOtaibi A. Comparison of polymeric cyanoacrylate adhesives with suturing in free gingival graft stability: a split mouth trial. Polymers (Basel) 2021; 13(20):3575. doi: 10.3390/polym13203575 [Crossref] [ Google Scholar]
- Agrawal E, Chopra R, Sharma N. Treatment of lingual gingival recession on mandibular lateral incisor using minimally invasive full-thickness tunneling technique and subepithelial palatal connective tissue graft. J Indian Soc Periodontol 2021; 25(1):78-82. doi: 10.4103/jisp.jisp_91_20 [Crossref] [ Google Scholar]
- Lee Y, Lee D, Kim S, Ku Y, Rhyu IC. Modified tunneling technique for root coverage of anterior mandible using minimal soft tissue harvesting and volume-stable collagen matrix: a retrospective study. J Periodontal Implant Sci 2021; 51(6):398-408. doi: 10.5051/jpis.2101400070 [Crossref] [ Google Scholar]
- Rimbert M, Barré R. New surgical approach for mandibular anterior root coverage by modified tunnel technique with simultaneous frenuloplasty: technical description and 5-year recall case report. Clin Adv Periodontics 2021; 11(3):155-60. doi: 10.1002/cap.10163 [Crossref] [ Google Scholar]
- Agrawal P, Katti N, Mohanty D, Pradhan SS, Raj SC, Satyarup D. Treatment of localized gingival recession using gingival unit grafts: an 18-month follow-up study. J Contemp Dent Pract 2022; 23(1):49-55. doi: 10.5005/jp-journals-10024-3276 [Crossref] [ Google Scholar]
- Alhourani MA, Kasem T, Hamadah O. Comparative study between using a tissue adhesive (N-BCA & OCA) and surgical sutures in free gingival graft surgery: a randomized controlled clinical trial. Dent Med Probl 2022; 59(2):241-8. doi: 10.17219/dmp/135382 [Crossref] [ Google Scholar]
- Tambe LV, Tandale MM, Chhibber R, Wu DT. Treatment of multiple gingival recessions using modified tunnel technique with V-reverse sutures: a report of three cases. J Contemp Dent Pract 2022; 23(2):232-6. doi: 10.5005/jp-journals-10024-3301 [Crossref] [ Google Scholar]
- Carcuac O, Trullenque-Eriksson A, Derks J. Modified free gingival graft technique for treatment of gingival recession defects at mandibular incisors: a randomized clinical trial. J Periodontol 2023; 94(6):722-30. doi: 10.1002/jper.22-0581 [Crossref] [ Google Scholar]
- Alrmali A, Saleh MH, Wang HL. Inverted T-shape free gingival graft for treatment of RT3 gingival recession defects: reporting of two cases. Clin Adv Periodontics 2023; 13(1):67-71. doi: 10.1002/cap.10231 [Crossref] [ Google Scholar]
- Danskin Y, Chu S, Simmonds T. Minimally invasive tunneling of a de-epithelialized connective tissue graft to improve gingival phenotype of lingual recession defects: a case report. Clin Adv Periodontics 2023; 13(4):235-40. doi: 10.1002/cap.10230 [Crossref] [ Google Scholar]
- Vilarrasa J, Blasi G. Double laterally moved coronally advanced flap combined with a connective tissue graft plus enamel matrix derivatives for the management of adjacent deep gingival recessions in lower incisors: a case report. Clin Adv Periodontics 2023; 13(1):62-6. doi: 10.1002/cap.10224 [Crossref] [ Google Scholar]
- Chang KJ, Mumford JH, Long A, Ton VH. Vestibular tunnel approach in restoring non-carious cervical lesion gingival recessions with combination of bioceramics and collagen matrix: a case report with a 1-year follow-up. Clin Adv Periodontics 2023; 13(1):56-61. doi: 10.1002/cap.10222 [Crossref] [ Google Scholar]
- Kashani H, Vora MV, Kuraji R, Fathi-Kelly H, Nguyen T, Tamraz B. Incision-free, coronally advanced flap with subepithelial connective tissue graft placed by the molar or canine access (MOCA) technique: 13 case series. Clin Adv Periodontics 2023; 13(1):11-20. doi: 10.1002/cap.10195 [Crossref] [ Google Scholar]
- Guimarães DM, de Andrade PF, Rebollal J, das Neves AM, Granjeiro JM. A modified tunnel technique to treat multiple gingival recessions: Case Series. Braz Dent J 2023; 34(3):136-45. doi: 10.1590/0103-6440202305502 [Crossref] [ Google Scholar]
- Deepika BA, Thamaraiselvan M. Comparison of modified suspensory suturing and anchoring suturing technique for gingival recession coverage by tunnelling and pouch technique. J Popul Ther Clin Pharmacol 2023; 30(10):e83-91. doi: 10.47750/jptcp.2023.30.10.013 [Crossref] [ Google Scholar]
- Santamaria MP, Rossato A, Miguel MM, Mathias-Santamaria IF, Nunes MP, Queiroz LA. Guided coronally advanced flap to treat gingival recession: digital workflow and case report. Clin Adv Periodontics 2025; 15(1):7-13. doi: 10.1002/cap.10282 [Crossref] [ Google Scholar]
- Yadav VS, Makker K, Haidrus R, Tewari N. A conservative approach for keratinized tissue augmentation: report of two cases. Clin Adv Periodontics 2025; 15(3):223-8. doi: 10.1002/cap.10309 [Crossref] [ Google Scholar]
- Rao TH, Johnson JJ, Malgikar S, Palaparthy RB, Basavaraju M, Gooty JR. Comparative evaluation of autologous fibrin glue and conventional sutures in the treatment of gingival recession using connective tissue graft - a randomised controlled clinical trial. Indian J Dent Res 2024; 35(2):181-6. doi: 10.4103/ijdr.ijdr_447_23 [Crossref] [ Google Scholar]
- Ambili R, Gopakumar D, Badarudhin BB. Free gingival graft embossed over laterally flipped periosteum for root coverage: a novel case report. J Indian Soc Periodontol 2024; 28(1):143-6. doi: 10.4103/jisp.jisp_447_23 [Crossref] [ Google Scholar]
- César Neto JB, Cavalcanti MC, Silva CO, Almeida VC, Sapata VM, Lazarin RO. Digital three-dimensional assessment of free gingival graft remodeling over 12 months. J Dent 2024; 148:105216. doi: 10.1016/j.jdent.2024.105216 [Crossref] [ Google Scholar]
- Skierska I, Górski B, Fus Ł. Tunnel technique and subepithelial connective tissue graft, with or without cross-linked hyaluronic acid, in the treatment of multiple gingival recessions: 12-month outcomes of a randomized clinical trial. J Periodontol 2024; 95(11):1060-72. doi: 10.1002/jper.24-0093 [Crossref] [ Google Scholar]
- Devkar N, Pudke S, Happy D, Dhamapurkar A, Deshpande M, Leggeri A. Modified coronally advanced tunnel technique (MCAT) for the treatment of multiple adjacent gingival recession (MAGR) using site specific de-epithelialized free gingival graft (DGG): a case report. Eur J Musculoskel Dis 2024; 13(1):83-90. [ Google Scholar]
- Lin GH. Double‐vestibular incision subperiosteal tunnel access (double-VISTA) with connective tissue graft for treating multiple gingival recessions: 2-year follow-up. Clinical Advances in Periodontics. 2025. 10.1002/cap.10333
- Yilmaz M, Türkmen E, Balci N, Toygar H, Çekici A. Comparison of free gingival graft and modified apical repositioned flap techniques to create attached gingiva: long-term (2 years) retrospective study. Bezmialem Sci 2024; 12(3):327-33. doi: 10.14235/bas.galenos.2024.58224 [Crossref] [ Google Scholar]
- Shakiliyeva S, Sahin D, Gunpinar S, Gursel M. Comparison of conventional and modified sling suture techniques in free gingival graft operations-a randomized controlled clinical trial. BMC Oral Health 2025; 25(1):279. doi: 10.1186/s12903-025-05456-x [Crossref] [ Google Scholar]
- Harris RJ. Clinical evaluation of 3 techniques to augment keratinized tissue without root coverage. J Periodontol 2001; 72(7):932-8. doi: 10.1902/jop.2001.72.7.932 [Crossref] [ Google Scholar]
- Katorza A, Horwitz J. Esthetic mucogingival treatment after biopsy of inflammatory fibroepithelial hyperplasia. Clin Adv Periodontics 2022; 12(3):175-9. doi: 10.1002/cap.10187 [Crossref] [ Google Scholar]
- McGuire MK, Scheyer ET. Randomized, controlled clinical trial to evaluate a xenogeneic collagen matrix as an alternative to free gingival grafting for oral soft tissue augmentation. J Periodontol 2014; 85(10):1333-41. doi: 10.1902/jop.2014.130692 [Crossref] [ Google Scholar]
- de Almeida VC, Pannuti CM, Ferreira MS, de Oliveira Lazarin R, Romito GA, Jung RE. Conventional versus flap-protected free gingival graft: a multicenter randomized clinical trial. Braz Oral Res 2023; 37:e001. doi: 10.1590/1807-3107bor-2023.vol37.0001 [Crossref] [ Google Scholar]
- Menceva Z, Dimitrovski O, Popovska M, Petrusevska G, Veleska-Stevkovska D. Free gingival graft in single and multiple soft-tissue defects. Res J Pharm Biol Chem Sci 2017; 8(3):1678-85. doi: 10.3889/oamjms.2018.127 [Crossref] [ Google Scholar]
- Azzi R, Etienne D. Recouvrement radiculaire et reconstruction papillaire par greffon conjonctif enfoui sous un lambeau vestibulaire tunnélisé et tracté coronairement. J Parodontol Implant Orale 1998; 17(1):71-7. [ Google Scholar]
- Zadeh HH. Minimally invasive treatment of maxillary anterior gingival recession defects by vestibular incision subperiosteal tunnel access and platelet-derived growth factor BB. Int J Periodontics Restorative Dent 2011; 31(6):653-60. [ Google Scholar]